Читать книгу The Body at Work: A Treatise on the Principles of Physiology - Alex Hill - Страница 9
На сайте Литреса книга снята с продажи.
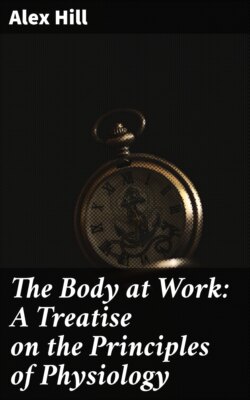
ОглавлениеFig. 4.—Red Blood-Corpuscles presenting, some the Surfaces, others the Edges, of their Discs, together with Single Representatives of Four Types of Leucocyte.
A, the most common type, highly amœboid and phagocytic. Its protoplasm is finely granular, its nucleus multipartite. B, a leucocyte closely similar to the last, but larger, and containing an undivided nucleus. It is shown with a cluster of particles of soot in its body-substance. C, a young leucocyte, or “lymphocyte.” D, a coarsely granular leucocyte. Its granules stain brightly with acid dyes—e.g., eosin or acid fuchsin.
Composition.—The structural composition of the blood, and the relation of its several constituents to each other, is best studied under the microscope. A thin transparent membrane in which blood is circulating through small vessels—the web between the toes of a frog’s foot, the mesentery, the membrane of a bat’s ear—affords an opportunity of observing blood in circulation. In any of the smaller vessels, whether artery or vein, a column of red corpuscles is seen moving in the axis of the stream. This column is surrounded by a layer of clear plasma. Amongst the red corpuscles a few leucocytes may be detected floating placidly down the current. Others are seen in the peripheral layer of plasma, tending to creep along the wall of the vessel rather than submit to be moved forward, as passive objects, by the current. If an irritant be applied to the membrane, the vessels dilate; yet, notwithstanding their wider calibre, the current becomes slower. The red corpuscles mass together. Apparently their constitution is slightly altered by this commencing inflammation, in such a manner that they cease to be clean, independent discs which slide past each other like small boats on a river; they exhibit a tendency to stick one to another. In the capillary vessels leucocytes may now be observed, not merely creeping along the inner surface of the endothelium, but squeezing themselves between its scales; making their way out of the vessel into the tissue-spaces through which the vessel passes. Such an observation gives the clue to the functions of the several constituents of the blood. The red corpuscles carry oxygen in chemical combination with their colouring matter. From them it passes into solution in the plasma; from the plasma through the walls of the capillary vessels into lymph; the tissues take it from the lymph as they require it. As fast as it is removed from lymph it is renewed from plasma. Carbonic acid excreted by tissue cells is dissolved in lymph. From lymph it is transferred to plasma. The reception of carbonic acid by these fluids is not quite so simple as the transference of oxygen from blood to lymph. It is aided by the presence of alkaline carbonates which are always ready to form “acid” salts: not acid to litmus-paper—the blood is always alkaline—but containing more than one unit of acid to one of base. Sodic carbonate has the formula Na₂CO₃. With an additional molecule of carbonic acid it becomes Na₂CO₃CO₂(HO)—bicarbonate. When in solution it can hold still more carbonic acid. If carbonic acid were merely dissolved in lymph and plasma, it would be impossible for the blood to carry it away with sufficient rapidity; just as it would be impossible for blood to bring sufficient oxygen were it not for the colouring matter (hæmoglobin) which forms a temporary, easily divorced union with it. But from a physical point of view it comes to the same thing. As the tension of oxygen in plasma falls, it dissolves more from the hæmoglobin. When the tension of oxygen in lymph is less than its tension in plasma, the former borrows from the latter. If the tension of carbonic acid in lymph is higher than in blood, it passes to the blood. The rapidly circulating blood at frequent intervals traverses the lungs. The whole blood of the body is exposed to air in the lungs once every minute. Oxygen tension being higher in pulmonary air than in venous blood, this gas is taken up. Carbonic acid tension being higher in venous blood than in pulmonary air, this gas escapes. The plasma in the capillary vessels which traverse the tissues exchanges gases with the lymph with very great rapidity.
The specific gravity of blood varies from 1·056 to 1·059. The corpuscles are heavier than the plasma. Its reaction to test-paper is alkaline, owing to the presence of bicarbonate of soda and disodic phosphate. The alkalinity is greatest when the body is at rest; it is diminished by severe muscular exercise. Blood contains about 5,000,000 red corpuscles, and 7,000 or 8,000 leucocytes, to a cubic millimetre. Red blood-corpuscles are biconcave discs destitute of nucleus, and, so far as can be seen, devoid of any investing membrane. Seen in profile they appear biscuit-shaped, because the centre is hollowed out. Their largest diameter is 7·5 micromillimetres (¹/₃₂₀₀ inch)—a measurement of great importance to anyone who works with a microscope, because it serves as a standard by which to estimate the size of other objects. They are soft, but fairly tough and highly elastic. In circulating blood a corpuscle may occasionally be seen to catch on the point where two capillary vessels unite. It bends almost double under the pressure of the column of corpuscles behind it, and then springs forward.
A red corpuscle is a vehicle for hæmoglobin. If blood is diluted with water, or if it is alternately frozen and thawed, the hæmoglobin separates from the corpuscles, which can then be seen as colourless discs. Hæmoglobin constitutes 40 per cent. of the weight of a moist corpuscle, or 95 per cent. of its weight after it has been dried. This is an enormous charge for a corpuscle to carry, and the question of how it carries it has been much discussed. It is not in a crystalline state. A corpuscle examined by polarized light is not doubly refractive. Microscopists know that if there were any crystals in the corpuscle it would appear bright on a dark ground when the Nicholl prisms are crossed. It cannot be in solution, since the water which the corpuscle contains would not suffice to dissolve it. It must be combined with some constituent of the corpuscle. But whether it is uniformly distributed throughout the disc, or in a semifluid form enclosed in spaces in a sponge-work; or whether the corpuscle is a hollow vesicle enclosing fluid hæmoglobin—a view which was long ago maintained, and has recently been revived—are questions which still await further evidence.
Red blood-corpuscles, properly so called, are found only in vertebrate animals, although invertebrate animals, from worms upwards, possess genuine blood, and in some of them it contains hæmoglobin, or a similar pigment in the form of globules. These might be likened to the non-nucleated corpuscles of mammals, but it must be remembered that the non-nucleated cells of mammals have been evolved from the nucleated blood-corpuscles of birds, reptiles, amphibians, and fishes. Below fishes red blood-cells are not found. Hæmoglobin is usually dissolved in the blood of invertebrate animals. It is impossible to trace any relationship between the coloured globules of invertebrates and the blood-cells of fishes. The coloured globules must be regarded as deposits or accretions of hæmoglobin held together by a proteid substance.
The nucleated red corpuscles of submammalian vertebrates multiply by cell division while circulating in the blood-stream. A good subject in which to look for dividing corpuscles is the blood of a newt in spring-time, when rapidly increasing activity calls for an additional supply. There is nothing to distinguish the method of division of a nucleated blood-corpuscle from that of any other cell.
The life-story of the red blood-corpuscles of mammals is one of the most fascinating that the histologist has to tell. He wishes that he could tell it with assurance; but, unfortunately, there are many uncertainties, due to conflicting testimony, in its earlier chapters. It is unlikely that a blood-corpuscle lives for long. A month or six weeks is probably the term of its existence. The rapidity with which the stock is replenished after bleeding shows that there must be ample provision in the body for making blood-corpuscles. The rate at which they disappear after they have been added in excess shows that there is an equally effective mechanism for destroying them. If half as many again as the animal already possesses be injected into its veins, the number is reduced to its normal limit in about ten days. It is clear that they can be made and can be destroyed with great facility, and it seems a legitimate inference that production and destruction are constantly taking place. Regarding the way in which they are destroyed there is no uncertainty. We shall refer to this subject when describing the functions of the spleen. But how are they made? We can sketch their history in outline, but the evidence is conflicting with regard to all matters of detail.
In early stages of embryonic life all red blood-corpuscles are nucleated, as they are permanently in birds and the other classes of vertebrates below mammals. In embryonic mammals they multiply by division whilst circulating in the blood, just as in the newt. But it is generally believed that this is not the most important source of new ones. During the earliest stages of growth they are being formed in enormous numbers. Such instances of division as can be seen in circulating blood appear to be all too infrequent to account for their rapid multiplication, and there can be no doubt but that a more complicated method of production is more important. Their formation is described as taking place “endogenously.” Certain cells termed “vaso-formative,” or “vaso-sanguiformative,” reach a considerable size, and become stellate in form, or branched. Their nuclei divide without the cell dividing. Each nucleus accumulates a little hæmoglobin round it. A space filled with fluid appears inside the cell. The nuclei project into this space. Then they drop off with their envelopes of hæmoglobin. The outer shell of the big vaso-formative cell becomes the wall of a capillary bloodvessel. By its branches it links up with other vaso-formative cells, making a network of vessels. The fluid inside it is the plasma of the blood. The nuclei and their envelopes are blood-corpuscles. This, if it be a true story, is a comprehensive way of making bloodvessels and blood at the same time. Doubts have been thrown upon its accuracy, but many leading histologists strenuously maintain that this description is correct.
At a certain period all nucleated red corpuscles disappear from mammalian blood. Non-nucleated corpuscles take their place. How are the latter formed? For a short stage of embryonic life nucleated cells containing blood-pigment are seen, or are supposed to be seen, in the liver—there is, unfortunately, great difficulty in distinguishing them with certainty from young liver-cells; later they are seen in the spleen; throughout the whole of life they are to be seen in the marrow of bone. The nucleated cells give origin to the non-nucleated corpuscles. It is hardly legitimate to call these cells persistent embryonic corpuscles. Yet the chain which connects the cells which in the embryo are capable of dividing into pairs of nucleated red blood-corpuscles, and the cells which, assuming the rôle of parent cells, do not accumulate hæmoglobin for their own purposes, but for the benefit of the red corpuscles which split off from them, is probably unbroken. In this sense they are persistent embryonic corpuscles which have deserted the blood-stream, and have taken shelter in certain tissues which are particularly favourable for cell division. The situations in which they hide themselves are singularly suggestive. In the liver there is an abundant supply of nutriment, more abundant than in any other part of the body of the embryo. Later, in the spleen, red blood-corpuscles are being destroyed. Materials available for making new ones must therefore be set free. The inside of a hollow bone is a peculiarly sheltered situation. The fat cells of marrow accumulate there after a time; but within some bones the marrow develops very little fat; hence it shows the red colour, which is due to its abundant bloodvessels. This “red marrow” is the most important seat of the manufacture of red blood-corpuscles in adult life. Unfortunately, when we try to answer the question, How are they formed? we are obliged to speak with caution. Some histologists assert that the nucleated cells divide, and that one of the two daughter cells accumulates hæmoglobin, and loses—that is to say, extrudes—its nucleus. Others maintain that the nucleated cells become irregular in form; that hæmoglobin accumulates in the projecting portion of the cell; that this projecting portion breaks off as a non-nucleated corpuscle. It would be indiscreet at the present time to pronounce in favour of either of these reports, although the decision is of theoretical importance. If the former account be true, red blood-corpuscles are nucleated blood-cells which have lost their nuclei. If the latter account be in accordance with fact, it is hardly justifiable to regard them as cells. They are parts of cells which finish their existence independently of the cell body and nucleus to which they belong. As circumstantial evidence, favouring the theory that cell division is normal and the nucleus subsequently lost, may be pleaded the existence in marrow, and also in the embryonic liver and spleen, of certain very peculiar cells. These cells have long been known as giant cells, and all attempts at accounting for them have broken down. They are relatively of immense size: their diameter may be twenty times as great as that of a red blood-corpuscle. Each contains a huge irregular, bulging nucleus. Hence the cells are termed “megacaryocytes” (big-nucleus cells). They must not be confounded with the polycaryocytes (cells with several nuclei), which eat up degrading bone, although it must be confessed that megacaryocytes and polycaryocytes appear to be genetically connected. It is supposed that megacaryocytes consume the nuclei which red corpuscles extrude during the process of their conversion from nucleated cells. Traces of nuclei, or things which often look like nuclei, are found in their body-substance. Their own overgrown misformed nuclei appear to be the result of an excess of nuclear food. It is certainly remarkable that megacaryocytes are not found below mammals. They do not occur in any animal in which red blood-corpuscles retain their nuclei. Polycaryocytes are found in numbers in the bones of growing birds. They are evidently scooping out bone from situations in which it has to be displaced in order that the shape of the bone as a whole may be changed. But there are no megacaryocytes in birds. On the other hand, megacaryocytes are present in the liver, and later in the spleen, of mammals at the periods when blood-formation is occurring most actively in these organs. From the liver they disappear early. In most mammals they disappear from the spleen about the time of birth; but in some—the hedgehog, for example—they are found in the spleen throughout the whole of life.
Hæmoglobin is a substance which has the property of uniting with oxygen to form oxyhæmoglobin—a compound from which the oxygen is, again, very readily withdrawn. It is extremely soluble, but may be made to crystallize by adding alcohol to blood, after setting the hæmoglobin free from the corpuscles by freezing and thawing. From the blood of Man and most other animals it crystallizes in the form of rhombic prisms, whether in the oxidized (oxyhæmoglobin) or non-oxidized condition. The addition of oxygen does not affect its crystalline form; although crystalline, it is absolutely non-diffusible. This is due to the great size of its molecule, which is probably larger than that of any other substance which is capable of crystallizing.
The percentage composition of hæmoglobin conforms closely with that of albumin and other proteins, with this most important difference: it contains a definite proportion of iron—0·336 per cent. That the percentage of carbon, hydrogen, nitrogen, sulphur, and oxygen should agree with that commonly found in proteins is inevitable, since it may be split into a part which contains all the iron, hæmatin, and a proteid part resembling albumin; and the latter constitutes 96 per cent. of its weight.
There is no doubt but that its value as a vehicle of oxygen depends upon the presence of iron. In the matter of taking up and dropping oxygen, hæmatin behaves somewhat in the same manner as hæmoglobin; whereas if iron be removed from hæmatin the “iron-free hæmatin” loses its respiratory value. It is almost certain that a molecule of hæmoglobin contains a single atom of iron. On this supposition its molecular formula may be calculated. It is not quite the same for all animals, although the variations are slight. For the blood of the horse it is as follows:
C₇₁₂H₁₁₃₀N₂₁₄S₂FeO₂₄₅.
This means a molecular weight of 16708. We give the figures, because the properties of hæmoglobin will be better understood if its prodigious molecular weight is borne in mind. In a sense, the reason for the great size of its molecule is not far to seek. The atomic weight of iron (Fe = 56) is much greater than that of either of the other elements contained in hæmoglobin. The molecule needs to be very great to float an atom of iron. As it is, the corpuscles are heavier than the plasma which surrounds them, in the proportion of about 13 to 12. Although hæmoglobin is a crystallizable substance, its immense molecule is absolutely non-diffusible. It cannot pass through a membrane. This is of no consequence as regards the relation of hæmoglobin to the walls of the capillary bloodvessels, since it is contained in corpuscles; but it is of great importance as regards its relation to the discs which carry it. A very small quantity of enveloping substance suffices to prevent it from diffusing into the plasma of the blood. The great molecules are held together and isolated from the fluid in which they float by a minimal amount of insoluble globin.
The iron needed for the making of hæmoglobin is obtained both from meat and vegetables. The constituents of an ordinary diet provide from 2 to 3 centigrammes of iron a day. The whole of the blood contains about 4·5 grammes. When corpuscles are being destroyed in the spleen, the iron which their pigment contains is largely reabsorbed and rendered available for further use. The iron in a mixed diet is more than sufficient to counterbalance any loss. Milk contains extremely little iron. Before birth the liver and spleen accumulate a store of iron which lasts until the end of the nursing period, unless this be unduly prolonged. If it be prolonged, the child is apt to become anæmic. Iron has been administered in the treatment of anæmia ever since its presence in the red clot of blood was recognized a hundred and fifty years ago. Physicians are agreed that in the anæmia of young people it is of value; but observations made with a view to obtaining definite data as to the increase in number of blood-corpuscles which results from the administration of iron, without any other alteration in the diet or the habits of the patient, have not given accordant results. Some observers have obtained an increase with organic compounds of iron, others with inorganic compounds; some are in favour of small doses, others of very large ones. As in the treatment by drugs of other abnormal conditions, it is difficult to isolate the effect of the drug from the effects of improvements in the general regimen. Yet physicians agree that iron accentuates the beneficial effects of fresh air and improved diet.
When the surface of the body is struck, the effect of the blow is marked at first by redness. There is nothing to show that small bloodvessels have been ruptured and blood effused beneath the skin. Next day the injured area is reddish-purple. The bruise turns blue, green, yellow, and eventually disappears. In the process of absorption, oxyhæmoglobin undergoes decomposition. First its proteid constituent is removed, leaving a coloured pigment containing iron, termed “hæmatin”; soon reduced by loss of oxygen to hæmochromogen. When Sir George Stokes first described the spectrum of blood (cf. p. 185), he showed that as hæmoglobin may exist in an oxidized and in a non-oxidized condition, distinguished by their spectra, so also may the coloured residue which is left after the proteid constituent has been removed from hæmoglobin. This coloured residue he termed, when oxidized, “hæmatin”; when not oxidized, “reduced hæmatin.” Stokes’s reduced hæmatin is now termed “hæmochromogen.” Hæmochromogen stands for the coloured nucleus of hæmoglobin. Although it is not present in hæmoglobin as hæmochromogen—hence we must not speak of hæmoglobin as made of a protein, x, plus hæmochromogen, y—it is to its coloured residue that hæmoglobin owes its value as a carrier of oxygen. Later, iron is removed from hæmochromogen, leaving hæmatoidin, a substance often found at the seat of old hæmorrhages, where it may remain unchanged for a very long time. Hæmatoidin is apparently identical with the yellow pigment of bile, bilirubin. The green colour which shows itself in the bruise seems to indicate that the more oxidized bile-pigment, biliverdin, is formed in the first instance. Red corpuscles, when destroyed in the spleen, pass through transformations similar to those which blood undergoes when effused beneath the skin. Their protein is used by the phagocytes which eat them. Their iron is reserved for the use of the blood-forming cells of the red marrow of bone. The pigment which remains as the residue of hæmoglobin is carried by the splenic vein to the liver, which secretes it as bile-pigment. So much of the bile-pigment as is reabsorbed by the wall of the alimentary canal is eventually excreted as the pigment of urine.
Such is the history of the changes which blood-pigment undergoes within the living body. To a certain extent its chemistry can be followed in the laboratory; but it must be remembered, when we are treating of the chemistry of a substance as complex as hæmoglobin, that the products which can be obtained from it in the laboratory are not necessarily those into which it is transformed in the body. In the laboratory oxyhæmoglobin is easily changed into methæmoglobin, a substance of the same percentage composition, but with its oxygen more firmly fixed. Methæmoglobin can be decomposed into a proteid substance and hæmatin. Hæmatin, when acted on by reducing agents, becomes hæmochromogen. Hæmochromogen, when subjected to such a reducing agent as a mixture of tin and hydrochloric acid, gives rise to coloured bodies closely resembling bile-pigments—not as they are secreted by the bile, but as they appear in the urine. It is impossible to prove that the changing colours of a bruise indicate a sequence of chemical transformations from hæmoglobin to bile-pigment, but it is not improbable that such a description is correct. The test commonly used to ascertain the presence of bile-pigment, i.e., bilirubin, is the play of colours which it exhibits when oxidized by fuming nitric acid. From yellow it turns to green, to blue, and then to purple, more or less reversing the colours of the bruise. It is fairly certain that effused blood undergoes changes along lines which, if not identical with those through which blood passes on its road to bile-pigment, are at any rate very similar.
Coagulation of Lymph and Blood.—Two or three minutes after blood has been shed it begins to clot. In ten minutes the vessel into which it has been received may be inverted without spilling the blood. After a time the jelly, holding all the corpuscles, shrinks from the sides of the jar. It squeezes out a transparent, straw-coloured fluid—serum. The clot continues to contract until, in a few hours, about one-half of the weight of the blood is clot, the other half serum. Lymph coagulates like blood, but most specimens clot more slowly, and the product is less firm.
When the process is watched through the microscope—a few drops of the almost colourless, transparent blood of a lobster afford an excellent opportunity of studying the formation of the clot—innumerable filaments of the most delicate description are seen to shoot out from many centres. They multiply until they constitute a felt-work. In the case of blood obtained from a vertebrate animal, this felt-work holds the corpuscles in its meshes. Its filaments exhibit a remarkable tendency to contract. They shorten as much as the enclosed corpuscles allow.
The filaments may be prevented from entangling the corpuscles by whipping the blood, from the instant that it is shed, with a bundle of twigs or wires. The fibrin collects on the wires, while the corpuscles remain in the serum. If this fibrin is washed in running water until all adherent serum and corpuscles are removed, it appears as a soft white stringy substance which, when dried, resembles isinglass.
Clotting is a protection against hæmorrhage. As it oozes from a scratch or tiny wound, blood clots, forming a natural plaster which prevents continued bleeding. It has little if any influence in resisting a strongly flowing stream of blood. But a clean cut through a large vessel is an accident which rarely happens as the result of natural causes. It is not the kind of injury to which animals are liable. When an artery is severed by a blunt instrument, the muscle-fibres of its wall contract. They occlude the vessel. The blood clots at the place where the vessel is injured, and plugs it. This happens also when a surgeon ties an artery. He is careful to pull the ligature sufficiently tight to crush its wall. His sensitive fingers feel it give. He stops before the thread has cut it through. As will be explained later, the clotting of blood is promoted by contact with injured tissue. If in tying an artery its wall be not crushed, the blood in it may remain liquid. When it is skilfully tied, the blood clots, forming a firm plug which is practically a part of the artery, by the time that the silk thread used in tying it is thrown out, owing to the death of the ring of tissue which it compressed. After a tooth has been extracted, the cavity is closed and further bleeding stopped by clotted blood.
When large vessels have been severed, the copious hæmorrhage which follows induces fainting. For a short time the heart stops, or beats very feebly. The blood-pressure falls. The bloodvessels contract. A clot has time to form. An emotional tendency to faint at the sight of blood is a provision for giving the various causes which stop bleeding an opportunity of coming into play. It is a useful reflex action, always supposing that the person who is liable to it faints at the sight of his own blood. Amongst other reasons for the greater fortitude of women—they are far less subject to this emotional reflex than men—might be alleged the circumstances of life of primitive people. It was the part of their women-folk to dress wounds, not to receive them.
The phenomenon of coagulation has attracted attention from the earliest times. It was a phenomenon that needed explanation, and culinary experience suggested analogies close at hand. Hippocrates attributed the clotting of blood to its coming to rest and growing cold. The blood which gushed from a warrior’s wound formed a still pool by his side. It set into a jelly as it cooled. Until the second quarter of the nineteenth century this theory was deemed sufficient. It then occurred to two men of inquiring mind to institute control experiments. John Davy placed a dish of blood upon the hob. William Hunter kept one shaking. In both experiments the blood clotted more quickly than it did in vessels of the same size, containing the same amount of the same blood, left upon the table.
Even before this date an observation had been made regarding the circumstances in which clotting occurs, which has thrown much light upon the causes of the phenomenon. In 1772 Hewson gently tied a vein in two places. At the end of a couple of hours he opened the vein. The blood was still liquid, but clotted in a normal manner after it was shed. Scudamore showed that blood clots more slowly in a closed than in an open flask. A new theory, as little trustworthy as Hippocrates’, was based upon these observations. Blood clotted because it was exposed to air. A record of all observations of the circumstances of coagulation, and of all the theories to which they have given rise, would make an exceptionally interesting chapter in the history of human thought. It would bring into singular prominence stages in the development of what is now known as the “scientific method.” Not that Science has a method of her own. Philosophers of all classes would follow the same method if their data allowed of its application. The peculiarity of the data with which Science deals is that they can be brought to a test of which the data of historical, or political, or economic theory are not susceptible. They can be confronted with control experiments. The control experiment is the alphabet and the syntax of the scientific method. No hypothesis is admissible into the pyramid of theory until it has passed this test. A natural phenomenon is observed. Every measurement which is applicable is taken and recorded—time, weight, temperature, colour. Scientific observation implies the tabulation of all particulars which are capable of statistical expression. Reflecting upon the relation of the phenomenon to other phenomena of a like nature, the philosopher—it is the philosophy of physiologists which interests us—formulates an hypothesis as to its cause. At this point the real difficulty of applying the scientific method begins. It is easy to formulate hypotheses. It is very difficult to devise control experiments. An experiment must be arranged which will provide that, while all other conditions in which the phenomenon has been observed to occur are reproduced, the condition which was ex hypothesi its cause shall be omitted. This digression into the philosophy of science may seem to be somewhat remote from our line of march, but it may perhaps hasten our progress in the comprehension of the story of physiology. There is no other science in which the control experiment plays an equally important part. Unless this is realized, the whole trend of experimental work will be misunderstood. Scudamore explained coagulation as due to contact with air. Based on the observations we have cited, no hypothesis could have seemed more reasonable. With a view to checking this hypothesis, blood was received into a tube of mercury. It coagulated in the Torricellian vacuum. Scudamore’s hypothesis, like many earlier and later, when confronted with a control experiment, was turned away, ashamed.
Clotting is a property of plasma. Red corpuscles play no part in the process. Coagulation does not occur in a living healthy vessel. It occurs when the vessel, and especially when its inner coat, is injured. It is hastened by contact with wounded tissues, especially with wounded skin. Contact with a foreign body also starts coagulation. If a silk thread is drawn through a bloodvessel, from side to side, fibrin filaments shoot out from the thread, as well as from the wound inflicted on the vessel by the needle which was used to draw it through.
Plasma contains a substance which sets into fibrin. It has been termed “fibrinogen.” It is present in lymph, and in almost all forms of exuded lymph. If sodium chloride (common salt) is added to plasma until it is half saturated—until it has dissolved half as much as the maximum quantity which it can dissolve—fibrinogen is thrown down as a flocculent precipitate. It can be redissolved and reprecipitated until it is pure. When fibrinogen was separated from plasma a step was taken towards the explanation of coagulation. Under certain conditions fibrinogen sets into fibrin. The question which then presented itself for solution was as follows: What is the substance which, by acting upon or combining with fibrinogen, converts it into fibrin? The clue to the solution of this question was obtained from the consideration of certain observations made by Andrew Buchanan in 1830, but long neglected, because their significance was not understood. Buchanan had observed that some specimens of lymph exuded into a lymph-space—the peritoneal cavity, for example—will clot; others will not. He noticed that they clot when, owing to puncture of a small bloodvessel during the process of drawing them off, they are tinged with blood. Determined to ascertain which of the constituents of blood is effective in rendering non-coagulable effusions capable of clotting, he added to them in turn red blood-corpuscles, serum, and the washings of blood clot. Either of the two latter was found to contain the clot-provoking substance. Thirty years later a German physiologist prepared fibrinogen from effused lymph by precipitating it with salt. He also treated serum in a similar way, precipitating a protein which he termed fibrinoplastin. When these two substances were dissolved and the solutions mixed, he obtained a clot, which he regarded as a compound of fibrinogen and fibrinoplastin. Subsequently he found that the mixture did not always clot, but he discovered that if he coagulated blood with alcohol, and washed this residue, the washings added to the mixed solution just referred to invariably produced a clot. Thinking that the substance which he obtained from his alcohol-coagulated blood could not be proteid, he termed it “fibrin-ferment.” He neglected the control experiment. He failed to ascertain whether or not all three substances were needed. Had he tried adding fibrin-ferment to fibrinogen, he would have discovered that the further addition of fibrinoplastin was unnecessary. He did not ascertain, as he might have done, that the weight of fibrin formed is somewhat less, not greater, than the weight of fibrinogen used. (Fibrinogen gives off a certain quantity of globulin when it changes into fibrin.) He was also wrong in supposing that the water which he added to alcohol-coagulated blood dissolved no protein. His “fibrin-ferment” is always associated with a protein. Since it may also be obtained from lymphatic glands, thymus gland, and other tissues which contain lymphocytes, it has been inferred that it is itself a protein, of the class known as nucleo-proteins. The fact that it is destroyed at so low a temperature as 55° C. has been supposed to confirm the theory that it is a protein. But with regard to the chemical nature of fibrin-ferment, as of all other ferments, we are at present in the dark. Under ordinary circumstances, when blood clots, the fibrin-ferment, or plasmase, or thrombin—it has received various names—is set free by leucocytes. Fluids which contain fibrinogen clot on the addition of a “ferment” which is either secreted by leucocytes or set free from leucocytes when they break up—as they are very apt to do, as soon as the conditions upon which their health depends are interfered with.
Freshly shed blood contains minute particles, termed “platelets,” in diameter measuring about a quarter that of a red blood-corpuscle. When the inner coat of a vessel is injured, platelets accumulate at the injured spot. They form a little white heap, from which coagulation starts. Evidently they supply the ferment, or a precursor of the ferment. As yet their origin has not been traced. They are too large to be the unchanged granules of granular leucocytes, but that they are in some way derived from leucocytes seems probable.
The further study of coagulation has shown that the conditions under which it occurs are more complicated than the simple explanation just given would seem to imply. This explanation holds good, so far as it goes, but facts connected with the details of the process have recently been brought to light which warn the physiologist that as yet his theory of coagulation is incomplete.
The presence of salts of lime has an important relation to coagulation. If blood is received into a vessel in which has been placed some powdered oxalate of potash, or soap, or any other chemical which fixes lime, the blood does not coagulate. All other conditions are as usual, but lime is withdrawn from the plasma. The non-coagulation of oxalated plasma was interpreted as indicating that lime, under the influence of fibrin-ferment, combines with fibrinogen to form fibrin; that fibrinogen altered by fibrin-ferment combines with lime. This hypothesis was based upon the analogy of the curdling of milk. Milk cannot curdle if lime be absent. If rennin (milk-ferment), prepared from milk from which lime has been removed, be added to a solution of caseinogen (the coagulable protein of milk), also prepared from lime-free milk, no curd is produced. The addition of a few drops of a solution of chloride of lime results in the immediate curdling of the mixture. Evidently rennin so alters caseinogen as to bring it into a condition to combine with lime. But the analogy does not hold good for blood. In the case of plasma, lime acts, not upon fibrinogen, but upon the fibrin-ferment—or rather upon a precursor of fibrin-ferment—in such a way as to render it effective. Leucocytes produce a prothrombin, which in contact with lime salts is converted into thrombin, which coagulates fibrinogen.
Fibrinogen is the substance which fibrin-ferment combined with salts of lime changes into fibrin. Yet even now the story is not complete, if the theory of coagulation is to be brought up to date. A perfectly clean cannula is passed into an artery of a bird. If it be thrust well beyond the place where the vessel has been cut, if the vessel be tied so gently as to avoid injury to its inner coat, and if the blood which first passes through the cannula be allowed to escape, the blood subsequently collected will not clot. It contains fibrinogen, lime salts, and fibrin-ferment, ordinarily so called; but the ferment is ineffective. The addition to the blood of a fragment of injured tissue, or of a watery extract of almost any tissue, immediately sets up coagulation. This observation brings fibrin-ferment into line with other ferments. Digestive ferments are secreted as zymogens, which require to be influenced by a kinase before they acquire fermentative activity. So, too, must thrombogen be changed into thrombin, under the influence of thrombokinase, before it can act upon fibrinogen. Almost all tissues yield the kinase which actuates fibrin-ferment. The utility of this provision is manifest. A bird’s blood contains everything necessary to form a clot with the exception of thrombokinase. The injury which brings the blood into contact with a broken surface supplies this ferment of the ferment. Fibrin-ferment, rendered active, at once changes fibrinogen into fibrin. The same interaction is necessary before the blood of a mammal is susceptible of clotting. But a mammal’s blood is even readier to clot than is the blood of a bird; for not only will a broken surface provide it with thrombokinase, but the leucocytes contained within the blood, when injured, also yield it. And the leucocytes are exceedingly sensitive of any change of circumstance; on the slightest indication that conditions are not normal they set free, perhaps owing to their own disintegration, the kinase which turns thrombogen into thrombin.
There is a constitutional condition, fortunately rare, in which blood does not coagulate. A person subject to this abnormality is said to suffer from hæmophilia. It is alleged that this condition is due to deficiency of lime in the blood; and the deficiency of lime is said to be due to excess of phosphates. The subject suffers from phosphaturia. His kidneys get rid of the superabundance of phosphates by excreting them in combination with lime. If this explanation be correct, there is a chronic insufficiency of lime in the blood, because it is being constantly withdrawn in the process of removing phosphates.
The difficulty in the way of establishing a complete theory of the coagulation of blood increases when the phenomena of incoagulability are considered. Blood may be rendered incapable of clotting in a variety of ways. Leeches and other animals which suck blood have the capacity of rendering it incoagulable. If the heads are removed from a score of leeches, thrown into absolute alcohol, dried, ground in a pepper mill, extracted with normal saline solution, a dark turbid liquor is obtained. This liquor, after filtration and sterilization at a temperature of 120° C., injected into the veins of an animal, renders its blood incoagulable.
The preparation sold by druggists under the name “peptone,” when injected into the veins of a dog, renders its blood incoagulable. Commercial “peptone” is a mixture of many substances. Its anticoagulation-effect is not due to the peptone which it contains. It has been supposed to be due to imperfectly digested albumin and gelatin (proteoses), but products of bacteric fermentation (toxins and ptomaines) are more probably the active bodies. Not only is the peptonized blood of a dog incoagulable, but if this blood be injected into the veins of a rabbit (an animal upon which the direct injection of peptone has no effect), it diminishes the coagulability of the rabbit’s blood. If peptonized blood be mixed in a beaker with non-peptonized blood, it prevents the coagulation of the latter. There is little doubt but that the poison, whatever it may be, acts upon the leucocytes; and there are some reasons for thinking that the poison is not contained in the “peptone,” but is secreted by the liver of the animal into which the “peptone” has been injected.
A still more remarkable property in relation to coagulation must be assigned to leucocytes. The blood of a dog which has been rendered incoagulable by injection of peptone recovers its coagulability after a time. If a further injection of “peptone” be made, the animal is found to be immune. Injection of “peptone” no longer renders its blood incoagulable. In a similar manner the blood develops a power of resisting the action of agents which induce its coagulation whilst circulating in the vascular system. Nucleo-proteins contained in extracts of lymphatic glands and other organs when injected into the veins of living animals cause their blood to clot, provided they are injected in sufficient quantity. If they are injected in quantity less than sufficient to induce coagulation, they render the animal immune to their influence. A larger quantity given to an animal thus prepared fails to take effect. This brings the phenomena of coagulation and resistance to coagulation to the verge of chemistry. They extend into the domain in which pathology reigns. Tempting though it be to record other facts with regard to these phenomena which recent investigation has brought to light, it is probably judicious to leave the problem at the frontier. Across the frontier lies a fascinating land, rich with unimaginable possibilities for the human race. Settlement is rapidly proceeding in this country, which is charted, like other border-lands, with barbarous names: “antibodies,” “haptors,” “amboceptors,” “toxins,” “antitoxins,” and the like—finger-posts to hypotheses which show every sign of hasty and provisional construction. But certain facts stand out, in whatever way theory may, in the future, link them up. The virus of hydrophobia, modified by passing through a rabbit, develops in human beings, even when injected after they have been infected, the power of resisting hydrophobia. The serum of a horse which has acquired immunity to diphtheria aids the blood of a child, which has not had time to become immune, in destroying the germs of this disease. It is a contest between the blood and offensive bodies of all kinds which find entrance to it, whether living germs or poisons in solution; with victory always, in the long-run, on the side of the blood, provided its owner does not die in the meantime. And not only is the blood victorious in the struggle with any given invader, but having repulsed him, it retains for a long while a property which neutralizes all further attempts at aggression on his part. In the past, physicians have fought disease with such clumsy weapons as mercury, arsenic, and quinine. Now they anticipate disease. In mimic warfare with an attenuated virus the blood is trained to combat. Smallpox which has been passed through the body of a cow is suppressed by the blood’s native strength. The exercise develops skill to deal with the most virulent germs of the same kind. In cases in which physicians cannot anticipate disease in human beings, they train the blood of animals to meet it; and, keeping their serum in stock, they can, when the critical moment arrives, reinforce the fighting strength of the patient with this mercenary aid.
The Spleen.—The spleen is placed on the left side of the body, and rather towards the back. It rests between the stomach and the inner surface of the eighth, ninth, tenth, and eleventh ribs. It is quickly distinguished from other organs by its brown-purple colour, a sombre hue to which it owed its evil reputation with the humoralists. The liver’s yellow bile tinged man’s mental outlook, preventing him from seeing objects in their natural brightness; but the spleen made black bile, which, mounting to the brain, displayed its malign influence upon the action of that organ, as, or in, the worst of humours.
The spleen is invested with a capsule of no great toughness. Inside the capsule is “spleen-pulp.” When the fresh organ is cut across, it is seen that, although most of the pulp is of the colour of dark venous blood, it is mottled with light patches. In some animals—the cat, for example—these whitish patches are small round spots, regularly arranged at a certain distance from the capsule. The distinction into “red pulp” and “white pulp” marks a division into two kinds of tissue with entirely different functions. The white pulp is lymphoid tissue, lymph-follicles developed in the outer or connective-tissue coat of the branches of the splenic artery. Its function is to make lymphocytes, of which, for reasons which will shortly appear, the spleen needs an abundant supply. The constitution of the red pulp is entirely different, and peculiar to the spleen. The branches of the splenic artery divide in the usual way into smaller and still smaller twigs until the finest arterioles are reached; but these arterioles do not give rise to capillary vessels. At the point at which in any other organ their branches would attain the calibre of capillaries, the connective-tissue cells which make their walls scatter into a reticulum. They are no longer tiles with closely fitting, sinuous, dovetailed borders, but stellate cells with long delicate processes uniting to constitute a network. The blood which the arterioles bring to the pulp is not conducted by closed capillary vessels across the pulp to the commencing splenic veins. It falls into the general sponge-work. The venules commence exactly in the same way as the arterioles end. Stellate connective-tissue cells become flat tiles placed edge to edge. The endothelium of an arteriole might be likened to a column of men marching shoulder to shoulder, three or four abreast; the connective tissue of the pulp, to a crowd in an open place. The column breaks up into a crowd. On the other side the crowd falls into rank as the endothelium of veins. The capsule and the red pulp are largely composed of muscle-fibres. These relax and contract about once a minute. By their contraction the blood is squeezed out of the sponge.
If the spleen be enclosed in an air-tight box (an oncometer), from which a tube leads to a pressure-gauge—a drum covered with thin membrane on which the end of a lever rests, or a bent column of mercury on which it floats—the pressure-gauge shows the changes in volume of the spleen. The long end of the lever, which records the variations of pressure in the gauge, may be made to scratch a line on a soot-blackened surface of travelling paper. A record of the variations in volume of the organ, which can be studied at leisure, is thus obtained. It shows that the spleen is sensitive to every change of pressure in the splenic artery. Small notches on the tracing correspond to the beats of the heart. Larger curves record the changes of blood-pressure due to respiration. A long slow rise and fall marks the rhythmic dilation and contraction of the spleen itself.
One of the three large arteries into which the cœliac axis divides delivers blood to the spleen direct from the aorta. The splenic vein joins the portal vein shortly before it enters the liver. Thus the spleen is placed on a big vascular loop which directs blood, not long after it has left the heart, from the aorta, through the spleen, to the liver.
The peculiar construction of the splenic pulp which brings the blood more or less to rest within its sponge-work, and the transmission to the liver of the blood which leaves the spleen, indicate that it is an organ in which blood itself receives some kind of treatment. It is not passed through it, as it is through all other parts of the body, in closed pipes. The spleen is a reservoir, or a filter-bed, into which blood is received.