Читать книгу Addicted to Christ - Helena Hansen - Страница 9
На сайте Литреса книга снята с продажи.
ОглавлениеIntroduction
BAPTISM
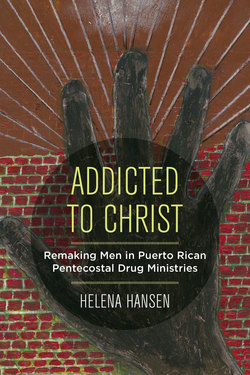
Pastor Mendoza1 stood in waist-high water. His face radiated sunlight, as did the pool that the ministry brothers had cleaned and filled that morning. The sun also warmed the pastel-painted walls of the ministry’s residence for ex-addicts. Together the pastor and the home director caught each of the newly born Christians as they crossed their arms on their chests, closed their eyes, and fell backward into the water (fig. 1). Brothers and sisters in Christ sank into the pool one after another, and onlookers clapped as they emerged. The cheering got a few decibels louder when the grandfather of the group—a thin, stooped man in his seventies—bent his arthritic knees to immerse himself in water. As he left the pool two young sisters wrapped him in a towel. His alcoholic tremor shook a drop of water from the tip of his nose.
FIGURE 1. A baptism at Victory Academy. Photo by Helena Hansen
I fumbled with my camera as Eli and Wanda chattered in the festive mood of the morning. They were discussing whether to get in line; neither wanted to be left out. Eli was dressed for the occasion in shorts, a loose T-shirt, and rubber sandals—clothes that she would not be permitted to wear at the Victory Academy on any other day, when exposed knees and toes were taboo. Wanda was less certain about baptism, as it would require her to change out of her long rayon dress. Meanwhile, Yeyo, the assistant director of the home, found a microphone and urged candidates to line up.
The pastor’s sons, playing synthesizer and drums, began singing “Libre, yo soy libre—¡Las cadenas del pecado han sido rota!” (Free, I am free—the chains of sin have been broken!)2 in an upbeat alabanza, a song of praise. Men gathered arm in arm, and started to brincar para Cristo (“jump for Jesus”) to the rhythm. Even the normally reserved wife of the pastor got carried away and began to hop in place. The band wound down with an adoración, a slow song of thanks. Tears streamed from the faces of a few brothers. A newly baptized man embraced the pastor, the tattoos on his muscular shoulders heaving with each silent sob.
Water baptism is a ritual of purification and consecration dating to pre-Christian Judaism. First-century Christians saw it as a reenactment of the death and resurrection of Christ. At this ministry, being reborn meant not only that the individual was no longer a marginal drug addict, but also that he or she joined the ranks of the privileged; the chosen. And that the chosen had an alternative addiction; one that—like drugs—altered their consciousness, heightened their senses, and provided moments of ecstasy, but—also like drugs—required total absorption and vigilance: an addiction to Christ.
Rings of onlookers surrounded the baptismal pool. Rebirth attendants stood knee deep in water preparing for delivery, lifting the heads and shoulders of the baptized from the water, one by one. Their vision was that those at the periphery of the pool would someday work their way toward the center, preaching, baptizing, and making room for new converts at the circle’s edge.
Even the building that housed converted ex-addicts embodied renewal. An abandoned motel destroyed in hurricane Hugo, ministry recruits had patched its walls, rewired its electrical system, and landscaped its grounds with flowers. In the ministry office, a photo of the motel’s crumbling entrance just after hurricane Hugo hung next to the current entrance, smoothed over with fresh plaster. On the motel’s exterior wall was a mural of a man, syringes littering the ground at his feet, his arms reaching up to a great cross.
THINKING AT THE MARGIN
Watching the baptism, it seemed that a natural experiment was unfolding in front of me. Working-class addicted people were attempting to take matters into their own hands, to create and invest in a form of life outside of narcotraffic. Some of them had converted days before, and were now only blocks away from the crack houses and heroin shooting galleries they had known. Yet, in the buoyant mood of the baptism, they seemed to be in another world.
This effort to create another world is the focus of this book. Clinical approaches to addiction presume an intrapersonal imbalance or deficit that must be corrected to return individuals to “normal” social functioning. In contrast, Victory Academy presumes that “normal” social functioning is itself corrupt, that it must be transcended through a transformation of the relationship between self and society and, ultimately, a transformation of society itself. My research for this book took me from society—recognizing street ministries as social movements that resist the logic of narcotraffic; to self—examining the individual spiritual practices of converts that enable them to resist; and back to society—the ways that self-making creates collectivities that redefine what is “normal.”
How do people with nothing make something? How do these people gain a sense of purpose, self-respect, and, ultimately, power?
The baptism at Victory Academy began to offer answers to questions that I had asked as an anthropologist and as a doctor who specialized in addiction; I was interested in the ways that people coped in the face of great odds. I knew that Puerto Rico’s narcotraffic was the result of a crisis of capital, just as it was in the decimated cities of the mainland United States. It was a crisis of post-industrial ways of life, of waning personal security, of lack of trust in the future, and of uncertain social reproduction. Lack of capital—not just economic, but also social, cultural, and symbolic capital (Bourdieu 1986)—leads to destabilization, displacement, and disengagement that further drains capital. This is the vicious cycle faced by Puerto Rican workers when manufacturing disappears, faced in U.S. inner cities when urban renewal and planned shrinkage policies dislocate residents, and faced globally by non-dominant religious and ethnic groups in the wake of war and disaster. In this vortex, homes are lost, neighborhood social networks are shredded, and disconnected individuals turn to addictive substances for momentary relief (Fullilove 2004, Saul 2013, Erikson 1976). Victory Academy attempted not only to heal individuals from loss, but also to create new collective capital.
In 2000, by the time I moved to Puerto Rico to begin field research street ministries like Victory Academy made up three-fourths of all substance-abuse treatment centers registered with the Puerto Rican state (Melendez et al. 1998). Rather than “treatment,” however, they offered a millenarian vision of redemption and transcendence of a corrupt world. Unlike clinics that identify biological or psychological predispositions to addiction, or that try to help patients to come to terms with traumatic memories, street ministries trained converts to fix their gaze forward and not dwell on the past. The only space they allotted for retrospection was in evangelical testimony, which contrasted past with present to narratively enact transformation and renewal. Converts were trained to cast old wounds aside, to shed them along with their pre-conversion selves.
My informants did not dwell on memories, but they were haunted by the lives they tried to leave behind. From my backroom conversations with Eli, at eighteen the youngest convert at Victory Academy, I learned of her childhood rape at the hands of her foster father. Each night Samaria, the leader of the women’s home, cradled Eli through violent nightmares. I knew that, the year before, Wanda had left her sleeping toddlers at home alone in search of heroin, and that she now traveled two hours to San Juan for court hearings to get them back from foster care. Yeyo, who had lost his job as a mechanic because of crack addiction, later opened an auto shop at the Academy to train young male converts in repairs. Yeyo’s ex-wife, skeptical of his conversion, disappeared with their sons. At the baptism, Yeyo was torn between his spiritual progeny in the ministry, and his compulsion to search for his sons. Additionally, despite Victory Academy’s promise to free women from abusive men, Eli and Wanda would find little room for themselves in the reinvented patriarchy of Victory Academy, where men were spiritual heads of home, and unmarried, willful women were a threat. Yeyo, Eli, and Wanda saw in the ministry a chance to renew themselves, to plaster over old wounds and build on firm ground. Unlike the motel that housed the ministry, however, the transformation of their identities and domestic lives was never complete.3
Incomplete transformations of social hierarchies are common in grassroots religious movements; examples include Muslim women’s attempt to forge their own leadership within the gendered structure of Islam, in places ranging from Egypt to African America (Rouse 2004, Mahmood 2004); and black Christian women’s church-based political activism and influence on male preachers (Frederick 2003, Casselberry 2017), and the blend of progressive and conservative politics reflected in African American televangelism (Walton 2009). Pentecostalism in particular historically has housed an array of gender and racial politics, ranging from Aimee Semple McPherson, single mother and preacher who founded Four Square Gospel, one of the largest Pentecostal ministries of the early twentieth century; and William Seymour, African American self-ordained pastor whose interracial 1906 Azusa Street revival was the progenitor of contemporary Pentecostalism; to televangelists Jimmy Swaggart and Jim Bakker, leaders of the anti-feminist and anti-integrationist U.S. Religious Right in the latter twentieth century.
Pentecostalism serves as an adaptable framework for social organization and cultural innovation, rather than being a stable set of practices, beliefs, or politics. To see its many valences, I provide foreground on the interpretations that converts make of themselves. I try to be cautious in applying theoretical frameworks that would give me narrative control, and am mindful of the words of social theorist bell hooks:
No need to hear your voice. Only tell me about your pain. I want to know your story. And then I will tell it back to you in a new way. Tell it back to you in such a way that it has become mine, my own. Re-writing you, I write myself anew. I am still author, authority. I am still [the] colonizer, the speaking subject, and you are now at the center of my talk (Hooks 1990, 241).
Narrative control can lead to colonization akin to that which contemporary anthropologists critique; it also can lead anthropologists to miss innovations occurring at social margins.
In medical anthropology, much of the contemporary ethnography of social margins builds on concepts of social suffering, in which an individual’s suffering is “taken as a manifestation of social structural oppression/or collective experience of cultural trauma” (Wilkinson 2005, Wilkinson and Kleinman 2016), as well as structural violence: the everyday violence of exclusion, deprivation, and vulnerability caused by institutional structures and policies that create inequalities (c.f. Scheper-Hughes and Bourgois 2004, Farmer 2005). These studies illuminate how power inequalities exact tolls on the bodies and minds of people on the margins. Global capitalist extremes of accumulation, deprivation, and war rob marginal people of their humanity. In post-industrial society, taken-for-granted bodily routines and popular discourses in themselves serve as technologies of control, theorized by Michel Foucault (1976) as biopower, in which people unwittingly reinforce their own domination as they manage and discipline themselves.
These bodies of work illustrate that individuals do not engineer their own marginality, but they leave open the question of how marginalized people can deliberately influence their own lives. Staying experience near to those at the bottom of social hierarchies, moral economy uses ethnography and popular history to theorize actions that appear self-destructive instead as acts of survival and resistance. Marxist historian E. P. Thompson (1971), who first elaborated the term “moral economy” in his study of the peasant bread riots of eighteenth-century Britain, and anarchist political scientist James Scott (1977), who popularized moral economy in his studies of Malaysian rice farmers, were both interested in peasant resistance to the encroachment of free market capitalism on the older systems of patronage and reciprocity that had ensured peasants’ subsistence. In the United States, urban ethnographers also contrasted the moral systems of the industrial poor with the dominant structures that threaten their survival. In the 1970s, anthropologist Carol Stack’s 1974 study of reciprocity among extended kin networks of African American women as a survival strategy challenged U.S. Secretary of Labor Daniel Patrick Moynihan’s report depicting black single mothers as the pathological producers of a culture of poverty.
In the decades that followed, urban ethnographers adopted moral economy as a framework to understand how some inner-city blacks and Latinos came to see the drug trade as honorable, and to analyze drug-use practices as based on reciprocity and solidarity (Reinarman 1979, Murphy 1987, Bourgois 1995). These studies highlighted their logics of survival, but concluded that these logics locked them into short-term strategies that ultimately maintained their oppression rather than changing the institutions that constrained them. This analytical approach has been enriched by post-structural ethnographers such as Cheryl Mattingly, who describes hope among the families of poor, severely ill African American children as an active practice rather than an emotion or attitude. For her, hope is “the practice of creating, or trying to create, lives worth living even in the midst of suffering . . . to forge new communities of care” (Mattingly 2010, 6). She considers “larger macrostructures as powerful cultural resources . . . that inform life on the ground, not as containers that enclose it” (Mattingly 2010, 47).
The view that marginalized people have developed specific practices of hope, or—in the case of the street ministries described here—technologies of transformation, challenges the idea that social suffering is passive. It raises the question of how marginalized people imagine other ways of living; how they enter the state of openness to new relations and directions described by philosopher Gilles Deleuze as “becoming” (Biehl and Locke 2010), and how they work “to construct a livable world on the other side of their experiences of contact and colonialism” (Robbins 2013, 459). Imagining other ways of living requires vision and action; it calls for moral entrepreneurs who can name, interpret, and dramatize the areas where social hierarchies are contested (Becker 1963), and for moral pioneers who can creatively draw on “prior social relations and cultural understandings [to] condition the uses . . . [of new] technologies” (Rapp 2011, 12).
The details of how people imagine and interpret their alternatives matter. In the United States (including Puerto Rico), the figure of the inner city black or Latino addict sits in the center of debates about whether poverty is culturally or structurally determined, and about the merits of “bootstrapping” and mutual aid as opposed to a systemic political-economic overhaul. Some call on the addicted poor to discipline themselves, to earn societal inclusion and respect. Others call for a reordering of the State to address unemployment and basic needs as fundamental causes of addiction. Few ask if and how addicted poor people already are positioning themselves for change. Within a U.S. political discourse that casts evangelical politics as a product of the conservative white middle and lower classes, the complex practices and motives of evangelists from non-dominant ethnic and racial groups rarely are examined.
Puerto Rican street ministries address the social and political marginalization of ex-addicted converts with a narrative of collective redemption and ascendance. Pentecostal ex-addicts cast themselves as the nidus for worldwide re-enchantment, as reflected in their written and oral histories of themselves. In these histories, addicts are the unlikely instruments through which the Holy Spirit redeems an apocalyptic reality, placing addicts at the center, rather than the margins, of world events. Ironically, Puerto Rico itself is both marginal and central to global political economies. It sits at the geographical and political margin between the United States and Latin America, its burgeoning narcotraffic is the product of the Puerto Rico’s rapid social transformation to meet the needs of U.S. national corporations, originally for low-cost labor and more recently as a primary corporate tax shelter. Puerto Ricans have U.S. citizenship and aspire to the living standards of the U.S. mainland, but do not control local capital. This creates the conditions for consumption of imports and for profound debt, and creates the political conditions to blame drug trade as the cause—rather than the result—of island-wide disinvestment. In this milieu, by 2000, the island’s transition to managed healthcare emerged as the flagship of Puerto Rico’s modernity and compatibility with U.S. mainland economy. Yet the governor—a physician—declared addiction a “spiritual-social” problem better addressed by faith- and community-based organizations than by biomedicine.
Street ministries raise questions about whether techniques of spiritual transformation are ultimately liberatory, whether they are complicit with domination, and whether liberation and domination are mutually exclusive. Here I track these questions through the attempts of a group of addicted, economically displaced Puerto Ricans to build spiritual power; to reinvent gender, family, and work in the alternate social order of self-fashioned ministries.
TRADING ON MORALITY
Ramón sat under the canvas awning that, with eight rows of rusted folding chairs and a makeshift altar of unfinished wood, marked the worship space at Victory Academy. As I studied the green tattoos that wound around his arms, his voice went up in pitch, he was silent for a moment. He was telling me about his daughters, born in the same year to two different women in a “crazy time” in his life, when he was injecting heroin.
His daughters, now nine years old, had shown up at his house wearing makeup. He made no comment. Instead, he grinned, “I played a trick on them.” He made them a big breakfast, then asked them to clean after themselves. When they said “But Daddy, we’re little, we don’t know how . . . ” he pointed to the Bible, “where it says ‘Everything in its time.’ I say ‘If you’re too little to clean, you’re too little to wear lipstick.’ ”
Although Ramón was not formally employed—his tattoos and criminal record made it difficult for him to get jobs—he was being discipled, that is, trained in spiritual leadership. “Now that I’m assistant director of the Academy, their mothers come to me for advice.”
Had Ramón made the transformation that people who are exhausted by addiction dream of? Was he—now an Academy director, trusted father and advisor—no longer an addict? Who is an “addict”?
In Puerto Rico, the people that I found in treatment for addiction did not mention withdrawal symptoms or the amounts of drugs they used when describing themselves as addicts. They described the moment that they lost their position in their families—of abandoning children and losing partners, or of being evicted from their parents’ homes—as the turning point in their self-perception as an addict.
When the Puerto Rican popular press describes addicted people, it shows depraved behavior around gendered roles in families. In the period of Ramón’s heroin use, daily newspapers ran articles with lines such as: “Addicts would even push their addicted sisters into prostitution to raise money for their fixes” (Suarez 1995). Such images were presaged by temperance-era discourses in which the voices of Puerto Rican feminist elites converged with those of local evangelists (as they did in Europe and North America), arguing that male Puerto Rican laborers caused their own poverty by drinking away their income and abandoning their families (Rosario Urrutia and Barcelo Miller 1989). A 1917 prohibitionist ad campaign in a Puerto Rican evangelical newsletter, for instance, featured a man on a barstool, chained to a bottle labeled “Slave to Rum,” while in his home his crying daughter says to her mother “I’m hungry. Why hasn’t Daddy come home?” (see fig. 2).
FIGURE 2. “I’m hungry. Why hasn’t Daddy come home?” Cartoon from Puerto Rico Evangélico, 1917.
Addiction is gendered and laden with power inequalities. Davis (1994) observed that a Latin American man is labeled an addict if he is unable to fulfill his role as family provider, lowering his stature in his community; although heavy drinking is socially sanctioned, addiction (defined as alcohol or drug use that interferes with upholding social responsibilities) is associated with moral weakness. In U.S. cities, the narcotics trade has long generated its own social hierarchy. Those at the top who sell but do not use, or who use but keep their use under control, claim moral and psychological superiority (Hanson, Beschner, Walters et al. 1985). The type of drug used, the method of use, and the source of income to pay for drug supplies also figure into hierarchies. Drug users have described crack cocaine smoking as more stigmatized than cocaine sniffing, impersonal theft as more ethical than theft from friends or family, and sex-for-drug exchanges between acquaintances as more respectable than street prostitution (Inciardi, Lockwood and Pottieger 1993, Rosenbaum 1981). Drug trade itself is structured around a motif of dominance and dependence, community respectability and stigma.
Domination and dependence also are recurrent motifs in Puerto Rico’s political history. Puerto Rico has been a U.S. possession since 1898; its people are U.S. citizens and are eligible for most U.S. federal welfare benefits. In the last two decades of the twentieth century, Puerto Rico saw 60% of its population qualify for welfare benefits, and had unemployment rates as high as 20% (Cockburn 2003, Chavez 1998, Buckley 1998). Its employment patterns and federal subsidies also led to a gender reversal in family economics. Puerto Rican men saw higher unemployment rates than that of women due to preferential hiring of women by international industries. Industries noted lower absenteeism, reduced union membership, and the acceptance of lower wages among women workers. Additionally, Puerto Rican women with children qualified more easily for federally funded public assistance than did men (Safa 1995a). Excluded from both legal industries and government entitlements, men disproportionately look to the illicit drug economy with its violently enforced hierarchies of power—from cartel leaders down to the addicted consumers subject to the vagaries of daily street supplies. Many men turn to the drug economy in hopes of gaining autonomy, but find themselves violently dominated by drug suppliers and by law enforcement. The drugs on which their bodies depend thus become a medium for political control by drug cartels and by the State.
With its connotation of dependence and lack of self-determination, a gendered analysis of narcotics addiction among unemployed Puerto Rican men could frame it as the post-industrial phase of what Edward Said (1978) called the feminization of the colonized, Oriental male. Although popular images of Latin American and U.S. urban drug traders portray their hypermasculine excesses of aggression and accumulation, they portray addicted men living in those places as powerless victims.
Street ministries offer an alternative, austere masculinity. Most of the addiction ministries I surveyed in Puerto Rico used no medication for withdrawal, not even Tylenol.4 Converts fast to build spiritual strength, putting the needs of the spirit before those of the body and relying on the Holy Spirit for sustenance. Where biomedicine works to eliminate pain, in Pentecostalism pain has spiritual value; it cleanses and strengthens. Within the Pentecostal logic, suffering is not a problem calling for relief. Suffering is a test of faith and a call to transcend the body.
These relationships with spirits, the way converts distinguish themselves through ascetic practice, and converts’ growing biblical knowledge are elements of what I call spiritual capital. In tandem with religious studies scholar Verter (2003), I adapt the construct from social theorist Pierre Bourdieu,5 who posited relationship-based social capital, as well as education and knowledge-based cultural capital, as forms of symbolic capital that are to some degree interchangeable with economic capital, and which enable the reproduction of social hierarchies from one generation to the next. Although Bourdieu’s formulations of capital focus on the strategies of the upper strata to maintain its position, I examine an alternative capital located in moral economies of the poor seeking to change their position. Critics of Bourdieu’s social capital theory question his assumption that the poor lack social capital (Lopez and Stack 2002). They broaden Bourdieu’s formulation of social capital by including non-mainstream social networks—such as those of churches—arguing that these alternative social assets and strategies are key for black and Latino communities because “the social capital that works through states and markets is not race-neutral” (Lopez and Stack 2002, 11).
Anthropologist Elizabeth Brusco (1995), writing of evangelical converts in Colombia, cites the “reformation of machismo” by their clean-living doctrine, which curbs male spending on alcohol, gambling, and extramarital affairs as a source of their upward mobility. Sociologist David Martin builds on this idea of alternate sources of capital to explain why Pentecostalism has won over so many converts from Catholicism in Latin America, writing that “Analysts of the post-modern city have referred without much exaggeration to the ‘impacted ghettoes’ and ‘ungovernable spaces’ of megacities. . . . This is where the domestic order and cleanliness of the Protestant, the secure family, and the church support systems create social capital out of nothing” (Martin 2002) (fig. 3 and fig. 4).
FIGURE 3. Evangelist with bullhorn in Ponce’s Town Square. Photo by Helena Hansen.
FIGURE 4. Billboard near Ponce: “I don’t question your existence.—God.” Photo by Helena Hansen.
Street ministries are self-help organizations in which ex-addicted sufferers become experts in their own healing. As ministry members progress, they gain authority and spiritual power, propagating themselves through a pyramid scheme of sequential recruitment and leadership. This contrasts with patients in biomedicine, who progress by submitting themselves more fully to the authority of medical professionals, becoming “compliant” or “adherent” patients. Across the Americas, a growing number of evangelical ministries are running residential drug-rehabilitation centers and gang recovery programs that address addiction (Flores 2013, Brenneman 2011).
The distinguishing feature of these ministries is their attempt to rework relationships. Converts are told to call on the Holy Spirit for spiritual strength to suffer through withdrawal and cravings, sleeping on bare floors, and feeding themselves on sparse donations from local stores. They are told to look to fellow worshipers for new “families in Christ” when their families of origin have rejected them, and to seek help from community congregations in order to live “por fe” or by faith alone—relying on donations and the ministries’ micro-industries (such as selling bottled water or chocolates on street corners). Although street ministries do not directly challenge the political systems and economic inequalities that produce narcotraffic, there are elements of the Pentecostalism of street ministries that serve as cultural critique. Ministries reject mass consumption and personal accumulation as a way to transcend the entrapments of popular culture.
Studies of Pentecostal rehabilitation in other parts of Latin America point to the influence of middle class white U.S. congregations and their neoliberal politics (O’Neill 2015), but many Puerto Rican street ministers see themselves as outside of worldly politics. Their discourse is otherworldly; converts renounce their bodily concerns to cultivate a connection to a dimension of spirits that gives them discernment—a way of perceiving and navigating the motivations and temptations of those around them. The less they rely on material comforts, the stronger their connection to spirits, the more elevated their consciousness and the more rewarding their emotional and sensory experience, as they become “addicted to Christ.”
This image of transferred addiction adapts a broader motif of rupture in Charismatic Christianity. Pentecostals urge adherents to break completely with the mundane, and to pursue salvation through contact with the Holy Spirit, marking a “split between the transcendental and the mundane [that] is thus as extreme in Pentecostal and Charismatic Christianity as it is in any other form of Christianity or in any other world religion” (Robbins 2009, 62). This split contrasts with other religions, many of which “are not structured around a radical distinction between the transcendental and the mundane” (Robbins 2009, 59). Thomas Csordas builds on this idea of rupture when asking about the broader social significance of the global Charismatic Renewal; “whether we are witnessing an era of re-sacralization or re-enchantment” (Csordas 2009, 91). In using the term “re-enchantment,” he alludes to Max Weber’s classic work on the Protestant work ethic as the cultural foundation for a modern secular capitalism. Weber points to the Calvinist doctrine of predestination as producing a psychological need of followers to appear successful as a result of their material labor to signal that they were saved (although perversely hard work and success were no guarantee of having been predestined for salvation). This compulsion to labor and produce good works carried forward in the industrial era and shed its Calvinist roots in contemporary, bureaucratic forms of life that are “disenchanted” in their reduction of human activity to a calculus of maximization (Weber 1958). Csordas argues that the popularity of Charismatic and Pentecostal Christianity can be explained, in part, by the ways that Charismatic worship is “imbued with an aura of enchantment;” by a sense of alterity that is heightened through practices such as speaking in tongues, and by the “sensuous immediacy” of revelatory visions and spirit possession (Csordas 2009). Tanya Luhrmann further illuminates this dynamic in her description of middle-class American evangelicals who walk and “talk with God,” who see their worship as a way to cultivate a personal relationship with God, a relationship that infuses the everyday with the mystical (Luhrmann 2012, Luhrmann 2004). The worshipers in her study therefore describe their enchantment as relational.
Despite the received wisdom that charismatic Christianity is centered on personal, inward transformation, rupture and re-enchantment are social processes. As Courtney Handman points out, Protestant missions have been associated with a “modernist refusal of sociality” with the ethos of individualism and private property of John Locke’s social contract. Yet, ethnographies of charismatic Christianity reveal a rich social matrix of worshippers attempting to enact authentic Christianity with and against each other (Handman 2015). Thomas Csordas’ (1994) classic ethnography of charismatic faith healing describes healers’ manipulations of memory and sensory phenomena to craft a “sacred self.” Although the goal is to transform selves, transformation requires carefully choreographed communication between supplicants and healers. The charisma, or gifts, of participants in these rituals are manifest due to the skills of healers and the concerted participation of other converts. Thus, the rupture and re-enchantment of Charismatic Christians are produced by collective practices (see also Comaroff 1985). But how complete is this rupture? Who ultimately benefits, and how?
This book examines the ways ex-addicted Pentecostals work toward rupture. One strategy for rupture is the performance of alternative masculinities. Having lost credibility with their families in the course of their addiction, converted men present themselves to their parents and spouses as spiritual heads of home. They draw on images of Christ to convert mainstream masculinity into an evangelical manhood that is based on domesticity, emotional responsiveness, self-sacrifice, and spiritual knowledge. This contrasts with the rise and fall of one of the only street ministries in Puerto Rico to cater to women. In their bid to cultivate the respectability and upward mobility of its male recruits, the ministries adopt a middle-class, patriarchal model of the family, over the working-class, female-headed extended families from which most of its membership comes, ultimately limiting the possibilities for women in the ministries.
I revisited several converted men and the outcome of their strategies of gender and domesticity two years after my original field research. Through these individuals we see that Pentecostalism—premised on the ultimate authority of personal, mystical experience—often is billed as an individualist replacement for extended family networks of the poor. In practice, however, Pentecostalism builds on these networks and its success is contingent on them. Together these chapters flesh out the promise and the limitations of Pentecostal strategies to rework gender and family as social technologies of transformation.
CHRONICITY AND CHANGE
Is addiction a disease?
Eight years after my research in Puerto Rican street ministries, in my last month of an addiction psychiatry fellowship, I was assigned to the inpatient addictions unit of a large New York City hospital. The staff hastily passed patients’ rooms, hovering two feet from the door. Thick glass insulated the nursing station from patients who frantically knocked on its window to ask for phone calls—and for sedatives.
I made a point of greeting a Puerto Rican woman who the medical assistants warned me was “unpredictable.” She was admitted the night before, had been sleeping all morning, but sat upright when I approached. Her hospital gown slipped off of her shoulder, showing skin as grey as the roots of her brassy hair. “Where is my methadone?!” she barked. Explaining that we hadn’t started morning medications, I caught her fist squarely in my chest, all she could muster from her withered arm. I froze, leaning toward her bed. Within seconds someone pulled me into the hall as medical assistants and nurses formed a circle around her. The crisis team appeared: African American former high school football stars hired from local housing projects. They told her she was going to get some rest, and held her to the bed as she screamed for methadone. A Filipino nurse injected her with tranquilizers.
Six hours later, nodding from the medications, she called me in to apologize. “I’m sorry about that—it’s just, you know, I need my methadone.”
My supervisor scolded me for walking so far into the patient’s room. “You see how the drug hijacks their brains.” In our classroom he had stood at the chalkboard, drawing dopamine receptors in the nucleus accumbens of the brain and its pathways to the forebrain, the seat of conscious decision making. He cited experiments derived from the behaviorist conditioning models of B. F. Skinner, describing the pleasurable reward of cocaine and heroin as “focusing us exclusively on pursuit of the drug, and making future oriented, cost-benefit analysis impossible.” It was an updated rendition of “Diseases of the Will” that historian Marianna Valverde (1998) had traced to Victorian doctors trying to account for addiction as a condition that took away self-control. Self-control, Valverde pointed out, was the distinguishing trait of humanity (as opposed to animal life) according to Enlightenment philosophy.
Biomedicine blames not only the substances, as Victorian temperance campaigns had, but also blames the individual’s genetic predisposition to addiction, and blames irreversible damage to the brain from long-term drug use. For instance, biomedicine’s “opiate receptor depletion hypothesis” proposes that chronic opiate use leads neurons to stop producing opiate receptors, to dampen the effect of high levels of opiates on neurons. This change explains why tolerance develops—that is, as the brain stops producing opiate receptors, higher doses of opiates are needed to achieve the same experiences of pain relief and pleasure. According to this theory, taking high doses of opiates daily over a period of years makes this down-regulation of opiate receptors irreversible: the brain permanently requires higher doses of opiates to control pain and feel pleasure. The brain stops responding to its own physiological opiates, such as endorphins, and without doses of external opiates such people live in a state of pain and anhedonia, unable to experience everyday pleasures. This is the principal neurophysiological argument for opioid medication maintenance with methadone or buprenorphine as a clinical treatment for opiate addiction.
My supervisor’s biological hijacking lecture came on the heels of President George H. W. Bush’s “Decade of the Brain” (1990–2000), a decade during which Congress allocated billions of dollars to the National Institute of Drug Abuse (NIDA) for neuroscientific studies of addiction as a “chronic, relapsing brain disease.” Addiction researchers and clinicians believed that conceptualizing addiction as a disease would reduce the stigma of addiction by mainstreaming addiction treatment into general medicine. The end of the decade was marked by a lead article in the Journal of the American Medical Association—authored by four prominent addictions researchers and entitled, “Drug Dependence: A Chronic Medical Illness” (McLellan et al. 2000). It argued that the heritability, etiology, and treatment adherence of addicted patients were similar to those of patients with diabetes, hypertension, and asthma, and that addiction should be treated in the same way (with medications) and in the same settings (in general clinics) as chronic physical illnesses. Addictions researchers hoped it would leave sufferers less stigmatized and with the more realistic goal of stabilization (instead of cure), than would a moral-deficiency concept of addiction.
In Puerto Rico—a U.S. territory that receives federal public-health funding—this biomedical view of addiction was making inroads. Two major universities near the capital city of San Juan had substantial NIDA funding for addiction research. State-funded biomedical detoxification and rehabilitation programs were firmly established and were being privatized in Puerto Rico’s move toward managed care. Most of the converts I met in Puerto Rican street ministries had tried biomedical addiction treatment, and many of the patients that I interviewed in biomedical programs had been in street ministries; biomedical and Pentecostal approaches thus were intertwined in their biographies.
Yet, biomedicine and Pentecostalism are rooted in different views of the self. In biomedicine, the addicted self is damaged, cannot regulate itself, and therefore cannot protect itself from further harm. Its closed loop of physiology and behavior is captured in biomedicine’s foundational “self-medication hypothesis,” the hypothesis that addiction is a faulty attempt to treat oneself with substances that relieve symptoms, but that simultaneously weaken one’s capacity for self-care (Khantzian 1985). The idea of self-medication infuses biomedicine’s primary addiction-treatment strategies to this day—from maintenance medications such as methadone that relieve the discomfort of withdrawal and mimic the action of illegal opiates, to cognitive behavioral therapy and dialectical behavioral therapy, designed to give patients non-pharmacological strategies to regulate their own distressing emotions. A more recent addition to this framework is the “Stages of Change” theory (Prochaska and DeClemente 2005) that identifies deficits in patients’ recognition of, and motivation to change, self-harming behavior such as addictive behavior. This theory has been combined with communicative strategies called “Motivational Enhancement” and “Motivational Interviewing” (Miller and Rollnick 1992). Physicians and therapists use these strategies to change harmful behavior by providing verbal reinforcements that are tailored to the patient’s stage of change, and are adjusted as the patient’s motivation and insight progress. In this way, willpower is directly bolstered by the clinician. To interrupt the addictive loop of physiology and behavior, therefore, biomedicine provides either pharmaceutical or psychotherapeutic prosthesis that enables addicted people to care for themselves. Prosthesis is the technology of hope offered by biomedicine: the hope of targeting neuroreceptors and psychological deficits that drive addictive responses by using precise molecular and psychotherapeutic techniques—techniques that, by the scientific master-narrative of progress, continuously improve with new breakthroughs over time, restoring self-dominion. According to biomedicine, however, the addicted self always will require psychosomatic technologies to adapt to the world. This cultural model calls on our investment in the pastoral care of individuals as a requirement for their everyday survival.
For their part, street ministries turn the biomedical view on its head. In the ministries’ frame, rather than helping addicted people to adapt to their environment, they call on people to remake their environment with spiritual techniques. Rather than accepting their powerlessness against their biology as “drug dependent,” ministries attempt to tap the power of a spiritual movement. Rather than asserting that addiction is a disease of the individual, ministries see it as a sign of societal disease. The goal is not to adapt to the world, but to create a new one. By this logic, prosthesis (such as medications or psychotherapy) only delay the liberation awaiting addicted people when they reject the world. The self is not permanently damaged; rather, the self is an embryonic seed, stunted by addiction, whose capacities must be cultivated with spiritual practice. This is in contrast to an inward-looking biomedical concern with inherited or historically shaped individual flaws; Pentecostal discourses of addiction are future oriented, calling on communities of worship and spirits as agents of change. The street ministry pastors that I knew had their own critique of biomedical addiction clinics, saying “You can’t cure drug addiction with drugs.”
As a prescriber of methadone and other medications used to treat addiction, I agreed with them. Drugs do not cure addiction. Yet, clinicians do not claim to cure, they only claim to manage a chronic disease (of addiction) with their medications. The most committed and skilled addiction doctors do help people to transform their lives, in part with medications that make withdrawal and cravings tolerable, medications that enable addicted people to face the complexities of family and work with less distraction.
Apart from a small, committed group of addiction specialists, however, most doctors are not eager to treat addicted patients. The chronic disease concept of addiction has only penetrated biomedicine so far. In both Puerto Rican and U.S. mainland medical schools, students and clinical residents run from patients who have “drug dependence” on their charts, delaying their admission exams for the next shift, or scanning their medical histories for reasons to refer them to a specialist. Addicted patients are non-compliant, have hidden motives, and are comorbid: sick with many diseases at once, including infections, liver disease, vascular disease, psychosis, and depression. They are the nemesis of overworked clinicians. Also, like many North and Latin Americans, clinicians often doubt that addicts deserve care.
In my own medical training, I was drawn to addicted patients. I pored over their social histories, convinced that they held the key to patients’ compulsions. I did find a pattern: almost all of these patients grew up neglected; were sexually, physically, or emotionally traumatized; or lived in violent neighborhoods, with unstable housing, pervasive unemployment, truncated schooling, and other deprivations. Population studies show that drug-use rates increase when industries leave local towns, or when people are forcibly relocated to reservations (Shkilnyk 1985) or to new housing projects under Urban Renewal (Fullilove 2004) or planned shrinkage (Wallace 1999) when extended family systems are broken apart by welfare eligibility policies (Pessaro 1993) or forced migration (Borges et al. 2007, Alaniz 2002), or when organized crime targets fragile neighborhoods for narcotics retail (Agar and Schacht Reisinger 2002). The flooding of inner-city drug markets by drug cartels selling cheap Columbian and Mexican cocaine and heroin, and the disproportionate incarceration of blacks and Latinos from the War on Drugs have converged with unparalleled toxic effects on city neighborhoods (Singer et al. 1992, Bourgois 1995, Hamid et al. 1997, Agar 2003, Singer 2008), visible in “million dollar blocks”: geomaps showing the low-income, black, and Latino census tracts whose residents cost the state the most due to high rates of incarceration (Badger 2015). Yet, nothing in my clinical training prepared me to treat addiction as anything other than an individual biological and behavioral problem.
In fact, some ethnographers argue that biomedical treatment that lacks a social perspective actually perpetuates addiction. Philippe Bourgois (2000) describes methadone programs as tools of neurochemical discipline that consign patients to long-term opioid maintenance upon pain of withdrawal. Angela Garcia (2010) followed heroin-using New Mexican Hispanos in addiction programs that, she discovered, are structured around the expectation of relapse—assuring the chronicity of addiction that they claim to treat. Summerson Carr (2010), in her linguistic analysis of group therapies, found that clients are forced to learn a “script” of sobriety to meet the expectations of their therapists, deepening the gap between their goals and those of their treaters.
As Wanda at Victory Academy told me, she preferred Christian treatment because “In the ministry they don’t say once an addict always an addict.” In this way, ministries diverge from another well-known spiritual approach to addiction, that of Twelve-Step programs such as Alcoholics Anonymous. In both evangelism and Twelve-Step programs, uncontrollable drug use is the consequence of a lack of humility and the need to submit to a higher power. Both require personal re-formation based on principles of the Bible (among charismatic Christians) or of the “Big Book” (among Twelve-Step followers). This similarity is not coincidental. In the 1930s, Alcoholics Anonymous co-founders Bill W. and Dr. Bob were members of the Oxford Group, a Protestant evangelical organization. Early on, Dr. Bob told hospitalized alcoholics to give their lives to Jesus (Dick B. 2005). The founders later expanded their membership by making the twelve steps non-denominational, and referencing a Higher Power rather than God (Valverde 1998). Yet, the Twelve Steps remain classic Protestant liturgy: admitting one’s shortcomings, turning one’s life over to a Higher Power, making reparations, and carrying the message to others (Alcoholics Anonymous 2004). The language has been secularized, but the steps refer to confession, salvation, penance, and evangelization.
At the same time, Twelve-Step programs identify addictions as incurable diseases that require sufferers to attend meetings indefinitely for sobriety, with the lifelong threat of relapse. This discourse of addiction as a disease of the individual was the product of a cultural compromise struck in post–World War II United States, in which Alcoholics Anonymous and the medical profession appeased public resistance to alcohol prohibition by attributing alcoholism to individual vulnerabilities, rather than the properties of alcohol itself (Peele 1989).
Although Pentecostal street ministries recruit and convert on the basis of problem drug use, addiction is not the primary issue to be addressed through conversion. As one convert told me, “The problem isn’t drugs or alcohol. The problem is sin.” Street ministry sermons give equal time to adultery, promiscuity, jealousy, and egoism; they place addicted people on the same plane as all unconverted people who need to align themselves with the Holy Spirit. For them, sobriety is not a goal in itself, it is the result of conversion.
The Book of Acts mentions faith healing as a gift bequeathed to early Christians during the Pentecost, along with speaking in tongues and prophecy, so faith healing—including prayer and laying hands on the ill with the expectation of their recovery—is widely practiced in Pentecostal ministries. Yet, I never heard street ministers speak of healing addiction. They measure their success not by the number of converts who return to their lives as they were before substance use, but by the number who devote their lives to the ministry, who live on the ministry grounds, who complete missions to other parts of the island or to other countries, and eventually open new ministry homes. Unlike Twelve-Step programs, whose twelve traditions forbid them to own property in the name of the organization, street ministries own, rent, or squat on properties that are full-time residences. In street ministries, conversion means gaining a new address, a new vocation, and a new identity.
Despite my biomedical training and my religious agnosticism, my own concept of addiction resonated with that of street ministers in unexpected ways. Where street ministers rallied to locate spirits, I saw a movement of people striving to relocate themselves. Where ministries made addicts into prophets, I saw social technologies of transformation. With the ministers, I wondered if the disease concept of addiction constrained the possibility of recovery. This paradox is highlighted by studies finding that defining addiction as a disease, rather than de-stigmatizing addiction as intended, can increase stigma against addicted people because the concept of disease casts them as irreversibly flawed (Pescosolido et al. 2010, Link and Phelan 2010).
My travels in street ministries required multiple ways of seeing addiction, and required holding the tension between a clinical gaze and ethnographic engagement. In a world where clinical medicine is dominant, where allopathic health care industries and pharmaceuticals represent the largest single sector of global industry (IMS 2012), I strove to understand strategies and ways of knowing that lay outside of biomedicine. How did conceiving of addiction as a spiritual disorder affect the possibilities for personal and social change?
PORTALS OF PENTECOSTALISM
By the end of the twentieth century, Pentecostalism was the fastest-growing religious movement in Latin America (Cleary and Stewart-Gambino 1997), having increased from 4% to 28% of the population between 1970 and 2005 (Pew 2006). In the early 2000s, Pentecostals were also the fastest growing Protestant denomination in the United States (Warner 2004). Pentecostals are characterized by the doctrine that any worshiper can establish direct contact with the Holy Spirit and receive its gifts as described in the biblical Book of Acts, including speaking in tongues, prophecy, and healing by faith. Pentecostalism gives ultimate authority to personal experience: to a communion with the Spirit that is available to all regardless of literacy, income, or previous knowledge of the Bible. As one worshiper in a Puerto Rican addiction ministry told me, “Pentecostals believe in personal sanctity, in long skirts and long sleeves. The experience of being saved is very clear, there is no doubt about the presence of God.”
Pentecostalism is not one denomination, it is a multi-denominational movement characterized by charismatic worship and a theology of gifts. Although many of the ministries I studied referred to themselves simply as Christian or evangelical rather than Pentecostal, I use the term Pentecostal because it describes a worship style that unites most of the street ministries in Puerto Rico.
Street ministries target beleaguered neighborhoods much like those of the early twentieth-century American cities from which Pentecostalism first emerged. Like the Azusa Street Mission of 1906 inner city Los Angeles, that unified African American, Mexican, and white American worshipers in what many historians identify as the first Pentecostal revival, contemporary Puerto Rican street ministries blend a clean-living doctrine of abstinence from substances and from sex outside of marriage, with an expressive worship style drawing on African and Latin American music and oratory, that is designed to elevate worshipers to a state of contact with the Holy Spirit.
The Pentecostal movement has deep roots in Puerto Rico, where Pentecostalism was well established by 1920, and produced several generations of Puerto Rican leaders and missionaries (Moore 1998). Notably, anthropologist Sidney Mintz’s classic 1950s biography of a Puerto Rican sugar-cane worker ends with the worker’s conversion to Pentecostalism (Mintz 1960).
Upon U.S. occupation of the island in 1898, the Catholic Church—which had been intertwined with the Spanish colonial government—no longer could exclude Protestant sects from missionary work on the island. North American Protestants rushed to missionize Puerto Rico, envisioning it as their portal to the rest of Latin America. Puerto Rico became a training ground for a Puerto Rican clergy who went on to found missions in the rest of Latin America (Milham 1951). Puerto Rico thus was evangelized earlier than its Latin American counterparts, due to its political and geographical proximity to the United States.
Early Protestant evangelists strove to solve problems of poverty and respectability in Puerto Rico. They opened hospitals and schools, and gained converts as a result (Sprinkle et al. 1964). Protestants supported temperance and prohibition; they identified widespread drinking among the rural poor as signs of moral depravity. The Protestant clean-living program—including abstinence from substances, legal marriage, and fidelity—appealed to Puerto Ricans looking for upward mobility (Martinez-Fernandez 2000). As in other parts of Latin America, Protestant conversion promised to affect male consumption and behavior—for instance, to reduce money spent on alcohol and mistresses—to elevate the image and income of their families (see Brusco 1995). Male abstention through Christian temperance therefore has been a recurring theme in Puerto Rican society for longer than it has throughout the rest of Latin America—where the Catholic Church was enmeshed with the state (Clark 1995).
In fact, in Puerto Rico (as in other former Spanish colonies) Pentecostals see themselves in opposition to Catholics, as an anti-establishment movement that challenges the rigid social hierarchy of Catholicism, and that challenges what they see as Catholicism’s empty moral pronouncements—the hypocrisy of lax personal practices among Catholic laypeople and clergy, who are said to drink alcohol and to be motivated by personal gain rather than spiritual connection. For Pentecostals, substances and material consumption detract from the spiritual authority of Catholics, whereas personal discipline builds the authority of Pentecostals.
Ironically, until the 1960s, many of these ascetic Pentecostal men worked in sugarcane fields, and thus helped to make Puerto Rico a major producer of rum for local consumption and for export to the United States. Beginning in the 1960s, however, Puerto Rico rapidly urbanized, becoming a manufacturing center for U.S. corporations seeking a lower-wage workforce and an import tax shelter. Later, as manufacturing plants sought even cheaper labor in Asia, Puerto Rico became a center of narcotraffic. As a U.S. possession, Puerto Rico’s customs procedures were minimal compared to those of other nations bordering the United States. By the 1980s—when the U.S. heightened narcotics surveillance at the Mexican border—Puerto Rico became the main Caribbean transfer site of Colombian cocaine and heroin to the United States (Abel 1998). Soon after, Puerto Rico saw a rate of injection drug use–related AIDS greater than that of New York City (CDC 2001), and a drug-related homicide rate greater than that of the mainland United States (Booth and Drummond 1996, Abel 1998, Goodnough 2003).
The baptism that I observed at Victory Academy took place in 2001, the dawn of the new millennium. The last quarter of the twentieth century had been punishing for families like Eli’s, Wanda’s and Yeyo’s. Lyndon B. Johnson’s War on Poverty had become what many called the War on the Poor. A key element in this shift was the War on Drugs, declared by Richard Nixon in 1971 to appease middle-class white voters shaken by black inner-city riots in Watts, Newark, Harlem, Detroit, Chicago, and Washington: voters anxious about alienated Vietnam veterans who had returned to an economy bankrupted by the war. The War on Drugs was intensified by Ronald Reagan starting in 1981 as he signed into law mandatory minimum sentencing for drug convictions, abolished parole for those convicted, and instituted the death penalty for “drug kingpins.” Since Reagan’s presidency, progressively more punitive drug-control legislation has been proposed every election year, leading, for instance, to disqualification of those convicted of a drug charge from receiving federal welfare or food stamps, even if disabled (Baum 1997). These laws coincided with structural adjustment in international economic policy, and national austerity in the United States: historic cuts in social welfare programs, industrial deregulation, growth in income inequalities, and growth in narcotics trade between Latin American and North America.
By the time I reached Puerto Rico, the effects of mandatory minimum sentencing for crack cocaine possession and targeted searches in poor neighborhoods across the U.S. mainland and territories were clear, with one in three black men and one in six Latino men in the United States serving time at some point in their lives (Maurer and King 2007). In the 1980s through the 2000s, U.S. Congress spent more than $600 billion total on supply-side drug control, including narcotics interdiction in the Caribbean, at the Mexican border, and through U.S. street-level arrests in the War on Drugs (Chalk 2011). In response, narcotraffic between Latin America and the United States grew more organized, technologically sophisticated, and murderous—becoming an industry of an estimated $100 billion per year in the United States alone (Kilmer et al. 2014). In the ten years since 2001, the War on Drugs led to more homicides in the United States than deaths in the wars in Iraq and Afghanistan (Conroy 2012). By 2011, Puerto Rico had almost twice the per-capita murder rate of Mexico (Latin American Herald Tribune 2012), and six times that of the mainland United States (Connor 2013), with more than 70% of homicides directly attributable to drug trade (Shoichet 2012).
Ethnographies of U.S. urban drug use and trade at the end of the twentieth century depicted them as alternative routes to income and respect among Latinos and African Americans excluded from capitalist mobility in the formal economy (cf. Williams 1989, Anderson 1990, Duneier 1999, Dei 2002). Instead, the excluded cultivate “oppositional identities” which reflect the skills and knowledge that are valued and rewarded in narcotraffic (Bourgois 1995). In those ethnographies, addiction was not seen as a problem of depleted opiate and dopamine neuroreceptors—what I had been taught in medical school—but as a problem of capital. In fact, in Puerto Rico, it might be more precise to describe widespread addiction as the result of, and a necessary condition for, shifts in the island’s economic base from agriculture and manufacturing to narcotraffic.
At the time of Victory Academy’s baptism, addiction also had other economic implications, accounting for more than 10% of U.S. health expenditures and 60% of prison sentences—to a total cost of $468 billion per year in the United States and Puerto Rico (CASA 2009, U.S. Department of Justice 2005). Both U.S. President George W. Bush and the Puerto Rican Governor Pedro Roselló ushered in the twenty-first century by espousing evangelism as a primary answer to drug abuse in the Americas, while many grassroots ministries resisted governmental support, seeing it as an encroachment on their practice of faith (Hansen 2005). The politics of addiction and evangelism were publicly debated, yet there was little sociocultural analysis of addiction ministries and the symbolic, relational, and political work they did for converts. Historically and to the present, we can see Puerto Rico—“Rich Port” in English—as a port of entry for Latin American narcotics and rum to the United States, and simultaneously as a port of entry for North American ascetic Protestantism to Latin America. In the crosshairs, the impact of street ministries’ efforts to reconfigure bodily practices, identities, relationships, and society has yet to be determined.
Puerto Rican street ministries strive to overcome addiction by re-imagining relations of power. This book begins by asking how spiritual transcendence, self-transformation, and enchantment of the world are cultivated in street ministries: that is, how Pentecostal healing of addiction “works” as a social technology. It ends by asking how these techniques ultimately influence a convert’s marginality—that is, if they “work.” I take up Pentecostal technologies of transformation that street ministries adapt to addiction: mysticism, ascetic practice, and the alternative power structure of ministries as “in the world but not of the world.” I then track converts’ gender-based attempts to establish moral authority in their ministries, their families, and communities. I end with elements of spiritual renewal and alternative community building that I recognized in the creative arts therapies and community gardening of a biomedical addiction clinic years after my research in Puerto Rico, elements that challenge the narrow pharmaceuticalization of addiction and mental health treatment. Pentecostal practices of identity change and re-valuation begin to answer the question to which I return at the end this book, of what clinical practitioners can learn and adapt from the other-worldly ministries encamped in Puerto Rico’s abandoned storefronts and motels.