Читать книгу Commentaries on the Surgery of the Npoleonic War in Portugal, Spain, France, - G. J. Guthrie - Страница 10
На сайте Литреса книга снята с продажи.
LECTURE V.
ОглавлениеTable of Contents
REMOVAL OF THE HEAD OF THE FEMUR, ETC.
84. The removal of the head of the thigh-bone from its place in the hip-joint, after it has been separated in a measure from its attachments by disease of a scrofulous nature, is an operation which has been several times successfully performed, and life has been thereby preserved without much suffering or risk to the patient. In this case, the head of the bone is found lying outside the cavity, from which it has been drawn by the action of the muscles. A step further must be taken, and this operation must some day be done in cases of fracture of the head or neck of this bone caused by an external wound—cases which have hitherto been invariably fatal, or in which life has been preserved by amputation at the hip-joint.
The great advance which operative surgery has made within the last forty years, and the success which has followed the removal of the head of the humerus, the whole of the elbow, the ankle, and even the knee-joint, render it imperative on surgeons of ability to endeavor to save life without the performance of so formidable an operation as that of the removal of the whole limb, more particularly when the health is good and the parts sound, with the exception of those immediately injured.
The cases which seem more particularly favorable for this operation are those in which the head or neck of the bone is broken by a musket-ball. Picture to yourselves a man lying with a small hole either before or behind in the thigh, no bleeding, no pain, nothing but an inability to move the limb, to stand upon it, and think that he must inevitably die in a few weeks, worn out by the continued pain and suffering attendant on the repeated formation of matter burrowing in every direction, unless his thigh be amputated at the hip-joint, or he be relieved by the operation which, I insist upon it, ought first to be performed.
85. In order to do this operation with precision, the surgeon should make himself well acquainted with the anatomy of the parts; and as the war in the Russian Empire may offer opportunities for its performance, a recapitulation of the essential points to be noticed may be useful. Two limbs should be injected so as to show the great arteries distinctly, and one should be dissected so that every part may be brought into view at once. That being done, attention should be directed to two points, the great trochanter and the round head of the thigh-bone in its socket, which is directly below and a little internal to the anterior superior spinous process of the ilium.
When the thigh is bent in the dissected limb, the head of the bone will be seen rolling in the socket very distinctly, and, in order to lay it bare for removal, the muscles, etc. around it must be divided. The first, on the anterior and outer part, is the tensor vaginæ femoris; this should be divided; outside this the gluteus medius must be cut, going to be inserted into the upper and outer part of the top of the great trochanter; deeper, and between these two last, lies the gluteus minimus, winding forward to be inserted into the anterior portion of the same part. Now, let the great gluteus muscle be cut through backward in a curve, and the insertions of four muscles at one part—viz., the pit or fossa immediately behind the great trochanter—will be brought into view: these are the pyriformis, the gemelli, reckoned as one muscle, and the obturatores externus and internus. They should all be cut through within half an inch from their insertion. The square muscle lying or placed immediately below them, and running from the ischium to the inter-trochanteric line, is the quadratus femoris; it must be cut across. The head of the femur will now be seen to roll in the socket on the least motion being given to the knee. The surgeon should then open into the exposed joint with great care, when by a gentle rotation of the knee inward the head of the thigh-bone will be readily dislocated outward. The ligamentum teres, or the round ligament, as it is termed, although it is triangular at its origin, should now be divided, with as much of the capsular ligament as may be necessary, when everything will be ready for the application of the saw.
Pause a moment, and view the parts before the saw is applied. Two strong muscles are inserted into the small trochanter by a common tendon, the iliacus internus and psoas magnus. This insertion should remain untouched if the fracture should not extend below the little trochanter. It is not always necessary to injure them, and they will be of great use afterward, if the operation should prove successful. If the neck of the bone be broken through, rotating the thigh as directed may not assist much in dislocating its head. But then, the separation of the fractured parts may be readily completed, and the piece detached, when the remaining part of the head of the bone will be more easily removed. The sawing may be accomplished with the greatest ease by a small common saw, or by the improved chain saw, which will do good service. The arteries to be divided are all of small size. Filled with red injection, they are so small as scarcely to be seen; and they could not give any trouble; for the wound is so large as to give easy access to every part, and readily admit of any bleeding vessel being tied without difficulty. The round ligament should be cut off close to its origin in the acetabulum, and any portion of the capsular ligament and cartilaginous edge of the acetabulum which can be quickly removed with it, but no time should be unnecessarily lost in trying to remove the cartilaginous lining of the cavity itself, which will be gradually absorbed. The sawn end of the femur should now be brought up into the cavity, and kept there if possible by a supporting splint and bandage, with the hope that it may become rounded and adhere by a newly-formed ligamentous structure, in the same manner as the end of the humerus does to the glenoid cavity of the scapula, when similarly treated. The edges of the wound are then to be brought in apposition, and retained so by two or three sutures. The gluteus magnus slides over the trochanter major, having a bursa between them, and this part will not readily throw out granulations. The surgeon may therefore be less solicitous about the accuracy of the apposition of the edges at the under part, through which the discharge will more easily pass. The outside must, however, be supported by sticking-plaster and bandage compress, to prevent any bagging, and to keep all parts in contact. The saving the periosteum of as much of the femur to be taken away, as strongly recommended by MM. Flourens and Baudens in the excision of the head of the humerus, should be attempted, although not easy of execution. (Aph. 118.)
86. The surgeon should now do the operation on the undissected limb. The first cut through the skin, integuments, and fascia lata should be a curved one, beginning just over the inner edge of the tensor vaginæ femoris muscle, as shown on the other leg, curving downward and outward, so as to pass across the bone an inch at least below the trochanter major, when it should turn upward to the extent of three inches or more, as the size of the limb may require. This incision or flap should, when complete, divide, in addition to the integuments, the fascia lata, the tensor vaginæ femoris, and part of the gluteus maximus. The flap thus formed must be raised or turned up by an assistant, to enable the operator to get at and divide the parts below, in the order before named. It is not necessary to stop to tie any bleeding vessel until the operation is finished, for little or no blood will be lost.
Pause again. The surgeon has just done nearly the outer half of the operation as to cutting, for removing the whole limb at the joint; and if he should now find that the bone is so much shattered in the shaft that he cannot hope to save the limb, there is no difficulty in removing it. To do this, place your long knife inside the bone, with the middle of its edge resting against the outer edge of the iliacus and psoas muscles, and at one firm cut of a strong hand let it cut its way inward, forming an inner flap, your assistant steadily compressing the femoral artery against the bone above. This artery and the great profunda will both be divided; seize them with the finger and thumb of the left hand, and place a ligature, or assist in placing one, on each branch with the right; or, if the trunk of the profunda should have been cut very short, tie the main trunk of the femoral. Let the ligature be a single thread of strong dentists’ silk, with which I have successfully tied the common iliac, and no fear need be entertained of its not holding fast if you tie it reasonably tight. The idea usually entertained that a great artery cannot be closed by the ordinary process of nature under a ligature, if a branch be given off near it, is erroneous. I never placed reliance on this opinion unless in the accidental circumstance of the outside of the orifice of the branch being in contact with the ligature, the irritation caused by which outside may not be sufficient to close the orifice within, and the common iliac artery of one of the two cases in which I tied it successfully (the patient dying a year afterward) may be seen in the Museum of the College of Surgeons. It is tied about an inch from the aorta, and was pervious on each side of the ligature, which has closed the vessel to no greater extent than its own width, proving all the facts I have mentioned so frequently on this subject. As to the smaller vessels, they will give no trouble, being easily commanded, each by the point of a finger. I have not done this operation of removing the head and neck of the femur on a healthy living man after an accident, but it must be done, and I am satisfied it will in the end succeed. It was done in the 3d Division of the army in the Crimea after the engagement of the 18th of June. The continuity of the head with the shaft was not altogether destroyed, the fracture being principally confined to the great trochanter and the trochanteric ridge. It was at first thought the operation might be dispensed with, but as great irritation ensued, with every prospect of considerable mischief, the head, neck, and both trochanters were excised. On the 6th of July the man was doing well, but unfortunately he was attacked by cholera three days afterward, and died. This operation has since been done by Mr. Blenkin, of the Grenadier Guards; the result will be stated hereafter.
Amputation at the hip-joint should not be performed, unless the head and neck of the thigh-bone be injured; and it ought not to be done if they be, unless the shaft of the thigh-bone be extensively broken also. The operation I have recommended should be its substitute, and I hope yet to see a man walking with ease and comfort on whom it has been performed. The recommendation thus given is the result of the experience of former times, of the whole of the war in the Peninsula and at Waterloo, matured by that of the last forty years in London hospitals, and by a due consideration of the state of surgery throughout all civilized Europe and America. Surgery is never stationary, and surgeons of the present day must continue to show that it is as much a science as an art.
87. Wounds of the knee-joint from musket-balls, with fracture of the bones composing it, require immediate amputation; for although a limb may be sometimes saved, it cannot be called a recovery, or a successful result, where the limb is useless, and is a constant source of irritation and distress after several mouths of acute suffering have been endured, to obtain even this partial relief from impending death. For one limb thus saved, ten lives will be lost; and the sufferer is often glad, after months and years have elapsed, to lose the limb thus saved, more particularly when the ball has lodged in the articulating surface of either of the bones. Amputation at a secondary period, in these cases, does not afford half the chance of success, for many will not survive the inflammation and the fever which will ensue. The amputation should therefore be immediate, unless excision can be substituted for it, and it is a point to be hereafter decided whether excision may not almost always be so substituted when the wound is made by a musket-ball, and the popliteal artery and nerve are not injured.
88. Compound fractures of the patella, without injury to the other bones, admit of delay, provided the bone be not much splintered. If the ball should have pierced the center of the patella, and passed out nearly in an opposite direction behind, the limb will not be saved. If the ball have struck the patella on its edge, and gone through it transversely, opening into the joint, it will very rarely be saved; but if it be merely fractured, there is hope under the most rigorous antiphlogistic treatment, and delay is proper. A ball will occasionally penetrate the capsular ligament, and lodge in the knee-joint, with little injury to the bones. If it cannot be extracted without opening extensively into the cavity of the joint, and the extraction of the ball is absolutely necessary, amputation or excision had better be performed at first, for it will be ultimately necessary. The condyles of the femur and the lower part of the bone being spongy, a ball may pass through them or between them, and fall into the knee-joint, or it may make a prominence on the side of the patella, without passing out, or immediately interrupting the motion of the leg, for the soldier may walk some distance afterward. The popliteal artery may also be divided in addition, and either of these cases will render amputation necessary, for the ball must be taken out on the fore part, and the general inflammation of the joint will either destroy the patient in a short time, or, after much distress and hazard, leave him no alternative but amputation. If a ball lodge in the condyles of the femur within the capsular ligament, and cannot be easily extracted, excision or amputation is advisable; for the limb, if preserved, will not be a useful one. If the ball, on the other hand, lodge without the capsular ligament, and cannot readily be extracted, the wound should be healed as soon as possible; and, although it may cause some little inconvenience to the knee-joint, the limb and life of the patient may be saved, as I have seen in many instances, when a continuance of persevering efforts to extract the ball would have exposed both to great danger. Many cases of wounds in the knee-joint, in which the capsular ligament has been wounded, and the articulation opened into without injury to the bones, do well, such as simple incised wounds made with a clean cutting instrument. The success attending all wounds of the knee-joint depends entirely upon absolute rest, upon the antiphlogistic mode of treatment being rigidly enforced, on the healthy state of the atmosphere, and on the locality being free from endemic disease. The limb is to be placed in the straight position, a splint to be put beneath it, in order to prevent any motion, and cold or iced water to be applied, especially in summer, to diminish the increasing heat. General bleeding may be had recourse to in sufficient quantity to keep all general inflammatory action in due bounds; but it is on local blood-letting that the surgeon must principally rely for the prevention of inflammation. Cupping can sometimes be performed with marked effect; but leeches are more serviceable when they can be procured in sufficient numbers; from twenty to forty, or more, may be applied at a time; whenever the sensation of heat is felt, and is accompanied by pain, they should be repeated until these symptoms subside. The necessity for the local abstraction of blood is so great that it should never be lost sight of for a moment; for if suppuration take place throughout the cavity of the joint, it is followed, in most instances, by ulceration of the cartilages and caries of the bones. By local and general bleeding, the application of cold, rigid abstinence, and the straight position, a recovery may sometimes be effected; but wounds of the knee-joint, however simple, should always be considered as of a very dangerous nature, infinitely more so than those of the shoulder, the elbow, or the ankle. When a poultice is applied to a gunshot wound of this kind, I consider it the precursor of amputation. Col. Donnellan, of the 48th Regiment, was wounded, at the battle of Talavera, in the knee-joint, by a musket-ball, which gave him so little uneasiness that he could scarcely be persuaded to proceed to the rear. At a little distance from the fire of the enemy, we talked over the affairs of the moment, when, tossing his leg about on his saddle, he declared he felt no inconvenience from the wound, and would go back, as he saw his corps was very much exposed. After he had stayed with me a couple of hours, I persuaded him to go into the town. This injury, although at first to all appearance so trifling, proceeded so rapidly as to prevent any relief at last being obtained from amputation, and caused his death in a few days.
89. Excision of the knee-joint is an operation formerly attended with so little success that it has been but rarely performed until lately. The result will, in all probability, be more favorable in cases of injury from musket-balls, in which the femur and tibia have both been much injured, without so much mischief being inflicted on the soft parts as would have rendered amputation necessary. In such cases, provided every accommodation, and particularly absolute rest and good air, can be obtained for the sufferer, excision should be attempted, in preference to the amputation recommended in 84 and 85. Some cases of success have lately been published by Mr. Jones, of the island of Jersey; some by Mr. Syme, Mr. Mackenzie, Dr. Gurdon Buck, Mr. Fergusson, and others. Mr. Jones’s method of operating is here transcribed, as sent to me by himself:—
“In my first case, the incisions were in this form H, two lateral, one along each side of the joint, and a transverse one immediately over the middle of the patella. The flaps were then dissected upward and downward, the patella removed—and I do not see that any advantage can be gained by keeping it, even if not diseased—the crucial and lateral ligaments were then divided, and the joint completely opened. The leg was afterward bent backward on the thigh, and the diseased portion of the femur was cleared, and removed with an ordinary amputating saw. The same method was followed with the tibia: the bones were then placed in juxtaposition, the flaps brought together by means of a few stitches, and the limb placed in a species of fracture-box. Water-dressing was applied. In the second case, I followed very nearly the same plan, with the exception of my first incisions, which were made something in a horseshoe shape. In the third case, I removed a considerable portion of integument, and, I conceive, with marked advantage. In the two former cases, I think the cure was protracted by preserving all the diseased external parts.”
Dr. Gurdon Buck, of the United States of America, in a case of anchylosis, with deformity, after a gunshot wound, removed the knee-joint by a transverse incision from one condyle to the other across the lower margin of the patella. A longitudinal incision intersected this, extending four inches above and below it. The flaps being dissected up, the joint was opened into by an incision across the ligamentum patellæ at the inferior edge of the bone, and also across the lateral ligaments. The adhesions of the articular surfaces were broken up by forced flexion very gradually applied. A slice was then removed with the common amputating saw from the surface of the condyles of the femur, including the pulley-like surface, care being taken to make this section on a plane parallel with the surfaces of support upon which the condyles rest, when the body is erect. The articular surface of the tibia was next removed on a level with the upper extremity of the fibula, after the insertions of the capsular ligament had been dissected up from the posterior half of the circumference of the head of the bone. The broad, fresh-cut bony surfaces, which were very vascular and healthy, admitted of accurate coaptation without stretching the tendons and other parts in the ham. To secure them in close contact, and prevent displacement, a flexible iron wire was passed through both bones on either side, and the two ends twisted and left out between the flaps of skin. The patella, being disorganized and softened, was removed, except the superior margin, which affords insertion to the quadriceps muscle. The flaps of integument having been trimmed, were brought together by sutures and adhesive plaster, and the limb placed in a fracture-box. The constitutional fever was moderate, and disappeared in a fortnight. Suppuration never exceeded half an ounce daily. At the end of five weeks and a half the wires became loose, and were removed. No exfoliation followed. At the end of nine weeks the wound had entirely healed, and the limb could be raised bodily from the bed. There is no mobility between the bones; the difference in the length of the limb, as compared with the other, is one inch and a half, which permits the foot to clear the surface of the ground, which cannot be done when the limb is of the same length as the other.
Mr. Jones, since the publication of his original cases, has in a subsequent one not only preserved the patella, but even the ligamentum patellæ, which he considers to be a great improvement when it can be effected; he operated in the following manner: A longitudinal incision down to the bone, four inches in extent, was made on each side of the knee-joint, midway between the vasti and the flexors of the leg. These two cuts were then connected by a transverse one just over the prominence of the tubercle of the tibia, care being taken not to cut the ligamentum patellæ. The flap was turned upward; the patella and its ligament were freed, drawn over the internal condyle, and kept there by means of a broad, flat, and turned-up spatula. The joint was thus exposed, the synovial capsule was divided as far as could be seen, when the leg was forcibly bent, the crucial ligaments, almost breaking in the act, only required a slight touch of the knife to divide them completely. The articular surfaces of the bones were now completely brought into view, when the diseased portions were removed by suitable saws, the soft parts being kept aside by assistants; the external condyle had been hollowed out by a large abscess, so that it was necessary to saw off (obliquely) another portion of the carious bone, and to gouge out the remainder, until the healthy cancellous structure was reached. The articular surface of the patella had also to be gouged until sound bone was attained. The bones were brought into apposition, and the patella and its ligament replaced, as nearly as possible; at the end of seven weeks the patient, twelve years old, was able to turn the limb from side to side, and ultimately recovered.
This little boy I saw walking firmly on his leg, an admirable instance of conservative surgery. It is, nevertheless, an operation which ought not to be done on the field of battle, unless perfect quiescence and every desired accommodation can be obtained, and no endemic disease prevail.
90. Amputation of the leg is performed in two ways—by the circular incision and by two flaps, the circular incision being only applicable to the calf. In either way the stump should, if possible, be seven inches long, for the more convenient application of an artificial leg, which is now made with a socket to fit the stump, instead of resting against the bent knee, unless the stump be too short for its proper adaptation otherwise.
The operation by the circular incision is performed by necessity in the thick part of the leg, and the bone is usually sawn through about four inches from the patella, so that, when the stump has healed, there may be sufficient length of bone left to support with steadiness the weight of the body on the knee, and that greater facility may be given to the motion of the leg, from the preservation of the insertion of the flexor tendons. The most eligible place for the application of the tourniquet, when used, is about one-third of the length of the thigh from the knee, on the inside, where the artery perforates the tendon of the triceps muscle, and where it can be most conveniently compressed against the bone by a small firm pad, the instrument being on the outside, or opposite the pad; or the compress may be placed between the hamstring tendons, a little distance from the hollow behind the joint, the instrument itself being on the fore part of the thigh. In this method the pad must be thicker, and the compression is more painful, and not more secure. The surgeon should stand on the inside of the leg to be operated upon, that he may more readily saw the fibula at the same time as the tibia, by which the chance of splintering the fibula is diminished; for this bone is held much more steadily under the saw when the tibia is undivided, whatever pains may otherwise be taken by the assistants to secure it. The limb should be a little bent, and the circular incision made with the smaller amputating knife through the skin and integuments to the bone on the fore part, and to the muscles on the outside and back part; and as the attachment of the skin to the bone will not readily allow its retraction, it must be dissected back all round, and separated from the fascia, the division of which in the first incision would avail nothing, from its strong attachments to the parts beneath. The muscles are then to be cut through, nearly on a level with the first incision, down to the bones. The interosseous ligament between the tibia and fibula is to be divided with the catlin; and as several of the muscles cannot retract in consequence of their attachment to the bones, they are to be separated with the knife; in the same manner the inter-muscular septa, or expansions running between them, are to be divided, as they would else prevent their retraction. The retractor with three slips is now to be put on, the center slip running between the bones, by which the soft parts may be pulled back to a sufficient distance, any adhering part being divided by the point of the knife. The bones are to be sawn through with the usual precautions, and the retractor removed, when the three principal arteries should be secured: the anterior tibial, on the fore part of the interosseous ligament, between the tibia and fibula; the peroneal artery behind the fibula; and the posterior tibial near it, more inward and behind the tibia; this artery will frequently, however, contract very much, and will only show itself on the compression being taken off the artery above. It in general causes more trouble to secure it than the others, and I have two or three times seen, even in London hospitals, the needle dipped round it in despair, when merely pulling out the artery with the tenaculum, and dissecting a little round it, would have shown the small retracted bleeding vessels arising from it, and have prevented, in all probability, a secondary hemorrhage. The tourniquet, if used, being removed, the smaller vessels tied, and the stump sponged with cold water and dried, the integuments and muscles should be brought forward as much as possible, and the strips of adhesive plaster applied from side to side—that is, the wound is to be closed vertically or nearly so, that the strips of plaster may not in any way press upon the fore part of the tibia, by which its protrusion will be avoided, an occurrence which almost invariably follows when the line of approximation is horizontal and the strips of plaster press upon the bone. If the spine of the tibia be sharp, it should be removed by the saw, whether the operation be done by the circular incision or by the use of flaps.
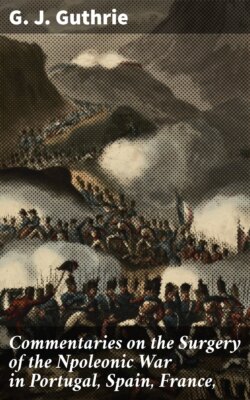
91. The flap operation, as performed by Mr. Luke, differs from that of the thigh in some particulars. There is a greater variety in the proportion which the soft parts in the posterior flap bear to those in the anterior, and the distance from the bones at which the limb is transfixed in the first step of the operation is subject to such variety that, when the calf is large, the mid-point for the introduction of the knife lies at some distance from the posterior aspect of the bones; in a small calf, it is close to it. The course of the knife through the limb is oblique instead of transverse, for the purpose of accommodating the line of incision to the plane of the two bones. The anterior flap is formed in the same way as in the thigh amputation, but it has proportionately more integuments and is thinner; yet its base and length are rendered equal to the base and length of the posterior flap, and may be adjusted evenly with it when the stump is dressed. In the circular division of the remaining soft parts, after the formation of the flaps, there is a necessary variation in the proceedings, from the circumstance of there being two bones united by interosseous membrane. It may, however, be accomplished by sweeping the knife around the more distant bone of the two, its point being afterward carried between the bones through the interosseous membrane. While the knife is between the bones, its edge may be so turned that the membrane may be divided longitudinally to any convenient extent for the easy introduction of a retractor, and the soft parts around the bone nearest to the operator may subsequently be divided by a sweep of the knife in a manner similar to that adopted for the division of parts around the more distant bone. The sawing of the bones and dressing of the stump are accomplished as in the thigh amputation; but more care is required to avoid pressure on the acute margin of the tibia, (which, when very sharp, should be removed,) and to prevent the pendulous state of the flaps.
A. The mid-point between B and C, at which the knife is introduced for carrying it across the limb. A to D. The course of the incision to form the posterior flap, E. F to g. The course of the incision to form the anterior flap.
When the nature of the injury renders amputation necessary at or immediately below the tuberosity of the tibia, the operation may be done with safety. Baron Larrey recommended the removal of the head of the fibula in such cases; I have done it with impunity, and thereby made a better stump than if it had not been done; but as the articulating surface of the head of the fibula does sometimes enter into the composition of the knee-joint, and as this cannot be known beforehand, the removal of this portion of the fibula is not advisable, neither must the tibia be sawn through above the tuberosity lest the capsular ligament be implicated. As an operation by which the knee-joint is saved, it is important; for although the stump is very short, it forms a solid support for the body, enables the patient to walk without the aid of a stick, and admits of the adaptation of an artificial leg. The skin, in these cases, must be saved in every direction by flaps, to form a covering. When in sufficient quantity, the operation may be done by the circular incision, as much muscle as possible being saved to aid in forming a covering on the under and outer sides. The posterior tibial artery will be found to have retracted behind the head of the bone, whence it, or others which may bleed, must be drawn out. The nerves should be cut as short as possible.