Читать книгу Commentaries on the Surgery of the Npoleonic War in Portugal, Spain, France, - G. J. Guthrie - Страница 14
На сайте Литреса книга снята с продажи.
LECTURE VI.
ОглавлениеTable of Contents
PRIMARY AMPUTATION, ETC.
102. An upper extremity should not be amputated for almost any accident which can happen to it from musket-shot; and there is scarcely an injury of the soft parts likely to occur which would authorize amputation as a primary operation.
103. If the head or articulating extremity of the bone entering into the composition of the shoulder-joint be merely or slightly injured by musket-shot, the arm ought to be saved with some defect of motion in the joint. The wound should be enlarged in the first instance, to allow of a sufficient examination with the point of the finger, and any loose pieces of bone should be removed. Inflammation is to be restrained within due bounds until suppuration has been established, when, if a clear depending opening should not exist for the discharge of the matter poured out, it should be made, and any loose portions of bone removed. The principal points to attend to are, the prevention of sinuses around the joint, by the formation of dependent openings, position, perfect quietude, due support, the methodical application of bandages, and occasional mild stimulating injections into the wound. A simple incised wound penetrating the joint, and even injuring the bone, does not call for any immediate operation. An attempt should be made to effect a cure by the first intention, which can only be managed by means of proper position and support.
104. If the head of the bone be much splintered, or if a ball have gone through it, that portion should be sawn off; for a part thus injured has often been a source of great inconvenience and suffering for many years afterward—during, in fact, the remainder of the life of the sufferer; which misery would have been avoided by the excision of the head of the bone in the first instance—an operation which ought in fact to be done even at a later period, if it had not been performed at the time when the injury was received. Secondary operations of this kind are never so successful as primary ones, and great discrimination should be exercised in attempting to save the head of the bone, or, in other words, to avoid the operation for its removal.
105. When the splinters extend far into the shaft of the humerus, it may be proper to amputate the whole extremity, especially if the great artery be also wounded; but the shaft is seldom broken in such accidents to any great extent, and amputation should be confined almost to injuries from cannon-shot or shells, or heavy machinery, destructive of the soft parts as well as of the bone.
106. When the injury done to the upper arm is so extensive that it cannot be saved, although the head of the humerus be not injured, the amputation should take place immediately below the tuberosities, and not at the joint, which latter operation always renders the shoulder flatter, and the appearance of the person more unseemly, than when the head of the bone is left in its place.
107. It will frequently happen that the arm may be irrecoverably shattered, and the thorax partake in a less degree of the injury, there being apparent only some slight contusion or grazing of the skin; if low down, the elasticity of the false ribs may have prevented the integuments being much injured in appearance, although the blow has been violent; yet the force of the large shot may have ruptured the liver or spleen. If higher up, it may perhaps fracture the ribs, in addition to a more severe contusion of the integuments. When these accidents occur, the symptoms arising from the wound or contusion of the trunk of the body are to be first considered. If they do not indicate a speedy dissolution of the patient, or the prospect of such an event in two or three days, the operation ought to be performed, and a chance of recovery given to the sufferer, which he would not have, the arm being retained, and the injury of the chest remaining the same. The danger to be apprehended in the more favorable cases is from inflammation, and this will be rather diminished than increased by the operation; the danger of deferring which is manifest and certain, while the injury committed in the thorax or abdomen is not ascertained, and its effects may be obviated. If the termination should be unfavorable, it can only be a matter of regret for the sake of the individual, and not for the non-performance of a duty. If the cavity of the chest be laid open, or several ribs beaten in, or a stuffing of the lungs take place from a large ruptured blood-vessel—all of which circumstances are obvious, and cannot be mistaken—the operation would, in all probability, be useless. A hemorrhage of short duration, or the expectoration of blood in moderate quantities, although a dangerous symptom, is not to be considered as depriving the patient of a reasonable chance for life, for it frequently follows blows from more common causes, from which many people recover. If the operation be delayed to ascertain what injury may have been done to the chest, from the symptoms that will follow, the danger resulting from both will be increased; and even when it has been ascertained that there is but little mischief existing in the thorax, the operation can no longer be performed with the same propriety, in consequence of the inflammation which has supervened; and the patient will probably die, when he would have recovered under a more decided mode of treatment.
108. A round shot or flat piece of shell may strike the arm, after rebounding from the ground, or when nearly exhausted in force, without breaking the skin, or only slightly doing it, yet all the parts within may be so much injured as not to be able to recover themselves: the bone may be considerably broken or splintered, the muscles and nerves greatly contused. The injury may not, perhaps, be quite so extensive. The bone may be merely fractured, and yet the soft parts will often be so much destroyed as not to be able to carry on their usual actions. A ruptured blood-vessel may, with an apparently slight external wound of this nature, pour out its blood between the muscles, and inject the arm to nearly double its size, all of which are causes rendering an operation necessary, and requiring decision, for inflammation will, and mortification may, ensue in a short time, when the most favorable moment for operation will have been lost.
109. Amputation at the shoulder-joint is an operation of little surgical importance. The fear formerly entertained of loss of blood has passed away, and every surgeon now knows that if he should happen to cut the axillary artery unintentionally, it can be held between the forefinger and thumb, without difficulty or danger, until a ligature can be placed upon it. No accomplished surgeon of the present day should give himself the least concern about compressing the subclavian artery. It is, on the contrary, better, when the arm is raised from the side preparatory to entering or using the knife, that the surgeon should then feel the pulsation of the artery in the axilla, that he may the more easily avoid, and subsequently command it. The axillary artery does not throw out much blood at each pulsation, and a little pressure with the end of the forefinger will always prevent bleeding, until the surgeon is prepared to take hold of the vessel with the tenaculum or forceps. The operator should, in fact, divest himself of all fear of hemorrhage. When gentlemen are afraid, however, and cannot help it, (for Henry IV. of France, ce roy si vaillant, always felt an inconvenient intestinal motion when a fight began,) compression may be made upon the subclavian artery by the thumb of an assistant, the round handle of a key, or the padded end of the handle of a tourniquet; the latter forms the best pad, and is usually at hand.
110. The great point to be attended to in performing the operation is to save skin to cover the stump. The directions, therefore, which are usually given for doing it after any particular method can only be occasionally useful; for the surgeon may not always be able to select the parts to be divided or retained. In cases of malignant disease of the bone and periosteum of the middle of the arm, my experience directs the removal of the whole of the bone at the joint, and not the amputation below the head; although the appearance of the integuments, and of the bone itself, would seem to encourage the attempt to preserve the roundness of the shoulder. In such cases, the removal of the extremity at the joint may be done by any one of the many ways which have been recommended for its performance. In none should the acromion or coracoid process be exposed, unless previously injured. Neither is it necessary to lose time, or to give pain, by depriving the glenoid cavity of its cartilage; but it should always be borne in mind that if the nerves be not shortened after the removal of the arm, they may be included in or adhere to the cicatrix, and cause, during a long life, much distressing pain to the sufferer.
111. Amputation at the shoulder-joint, performed immediately after the receipt of an injury, is now a very simple operation, for which simplicity English surgery is also indebted to the Peninsular war. As a secondary operation, or done at a later period, when the parts are all impacted together, it is less so. In both stages it is absolutely necessary to remember—1st. That, except in cases of disease, and not of injury, the shaft of the bone must be broken; and that all the directions usually given for rotation of the arm inward and outward during the operation are unnecessary cruelties not to be attempted, and rarely to be effected if attempted, with a broken bone. 2d. That the arm should always be raised from the side and supported by the hand of an assistant, who can feel, if he please, at any time of the operation, the pulsation of the axillary artery; and all operative methods are hereby condemned in which this precautionary measure is not the first step.
112. Operation by two flaps, external and internal.—The outer—beginning nearly an inch below the acromion process, the hair in the axilla having been previously removed—is to be carried down with a gentle curve so deeply as to divide the deltoid muscle, and to show the long head of the triceps at its under and outer edge. The second incision is to be carried in a similar direction on the inside, through the deltoid muscle, but need not divide the insertion of the pectoralis major, which should be exposed. These flaps being held back, the joint will be seen and readily opened into at its upper part, by cutting upon the head of the bone, in doing which the long tendon of the biceps will be divided, allowing the head of the humerus to drop from the glenoid cavity sufficiently to admit the forefinger of the left hand, on which the supra-spinatus, infra-spinatus, and teres minor may be cut through externally, as they go to be inserted into the great tuberosity, and the thick tendon of the sub-scapularis muscle internally, where it is attached to the smaller tuberosity. The head of the bone is then readily drawn out from the glenoid cavity, when the inner flap, including the axillary artery, vein, and nerves, may be taken hold of between the two forefingers and thumb of an assistant, while the surgeon, with one sweep of the knife, divides all the remaining parts below. The axillary and the posterior circumflex arteries will have to be secured; the anterior circumflex, when arising from the posterior, is frequently cut off with it; the nerves are to be shortened; the flaps brought together by sutures; and an especial pad placed upon the pectoralis major, to prevent unnecessary retraction, if possible.
113. The operation by one, or nearly one upper flap, is to be performed when the under soft parts of the arm have been destroyed, and the bone broken. It may be done by thrusting a small, two-edged knife through the integuments and under the deltoid muscle, from side to side, to form a flap; or it may be made by commencing an incision an inch above the posterior fold of the armpit, and carrying it over the arm in a curved form, the convexity being downward, to the same height on the anterior fold; the lowest part of the incision being five fingers’ breadth from the point of the acromion, the posterior end or point of it being somewhat higher than the anterior one. The flap being turned up, and the tendon of the pectoralis major divided, the head of the bone is to be exposed and separated as before stated, as much as possible of the integuments being preserved on the under part of the arm. This will often be best done by dissecting out the head and broken pieces of bone, and then preserving in succession every piece of sound integument, before the artery, vein, and nerves are divided.
114. Lisfranc and many French and continental surgeons recommend the operation to be done with a pointed, double-edged knife, in the following manner: The arm being approximated to the trunk, in a state of half pronation, the point of the knife is to be entered at a small triangular space, which may be perceived on the inside of the fullness of the shoulder, bounded above by the scapular extremity of the clavicle and a small part of the acromion; on the inside, by the coracoid process; and on the outside, by the head of the humerus. The knife thus entered obliquely is to be passed across to the outside, opening in its passage into the joint, when, by sliding the knife forward over the head of the bone, while the deltoid is raised up by the operator or an assistant, a flap is to be formed, during which proceeding the arm is to be raised from the side, to facilitate its performance. If this flap be well made, the upper part of the capsular ligament, the tendons of the long head of the biceps, and the supra-spinatus are divided, and the tendons of the infra-spinatus, teres minor, and sub-scapularis are also cut through in part, if not entirely. The upper and posterior flap is thus completed.
In the second step of the operation, the surgeon passes the knife behind the head of the humerus, and makes the under and anterior or inner flap, by cutting downward and inward, including in it a very small portion of the deltoid, the pectoralis major, latissimus dorsi, teres major, the triceps, coraco-brachialis, the short head of the biceps, and the vessels and nerves, when the limb is separated from the body. The flaps are nearly of the same size, and are to be brought together by sutures.
In the secondary operation, or that done several weeks after the receipt of the injury, in consequence of the attempt to save the arm having failed, it should be borne in mind that the soft parts will often be found so altered and impacted together that they will not yield or separate; and nothing is gained but by each cut of the knife, causing thereby some little delay, inconvenience, and loss of time.
115. Amputation of the arm immediately below the tuberosities of the humerus ought to be done in the following manner: The arm being raised from the side, and an assistant having compressed, or being ready to compress, the subclavian artery, the surgeon commences his incision one or two fingers’ breadth beneath the acromion process, and carries it to the inside of the arm, below the edge of the pectoral muscle, then under the arm to the outside, where it is to be met by another incision, begun at the same spot as the first, below the acromion process. The integuments, thus divided, are to be retracted, and the muscular parts cut through, until the bone is cleared as high as the tuberosities. The artery will be seen at the under part, and should be pulled out by a tenaculum or spring forceps, and secured as soon as divided. The bone is best sawn, the surgeon standing on the outside; the nerves should be cut short, and the flaps brought together by two or three silk or leaden sutures. There are few or no other vessels to tie, and the cure is completed in the usual time, while the rotundity of the shoulder is preserved. This operation is similar to that already recommended for the amputation at the joint, which in many cases it is intended to supersede.
116. Excision of the head of the humerus.—The point governing the modus operandi of this operation is, and ought to be, the fact that, under the most favorable state of recovery which can take place, the shoulder-joint usually becomes so stiff that its ordinary motions may be considered to be lost. Operative processes which have for their principal object the sparing of the deltoid muscle are unnecessary, for, if spared, it is as useless as if it had been cut; and it seems to have been forgotten that, when cut, it reunites, and becomes nearly as strong as before it was injured. It is the joint that cannot be moved, not the muscle which has lost its power. I prefer, therefore, in doing this operation, in cases of some standing, to make a short crescentic flap by an incision across the anterior part of the shoulder, as in the operation of amputation, which, on being turned up, leaves the joint exposed. The edge of the knife being applied to the head of the bone in a line below, but immediately under the acromion process, divides the capsular ligament, and with it the long tendon of the biceps, on which the arm drops from the socket, or glenoid cavity, and allows the finger to be introduced, when the three muscles inserted into the great tuberosity may be cut through, and the sub-scapularis inserted into the small tuberosity will also be divided. The head of the bone is then readily brought out, and may be easily detached from any surrounding connections, and sawn off with little or almost no loss of blood. The elbow is to be supported, so as to bring the end of the sawn bone in apposition with the glenoid cavity. The flap may be allowed to unite with the parts below as soon as it will, the shot-holes, if any, being in general sufficient to allow of such discharge as may be necessary.
In cases of recent injury, considerable aid will be obtained in keeping the sawn end of the humerus in apposition with the glenoid cavity, by not dividing the long tendon of the biceps. This must be done by dissecting it out of its groove in the humerus, between the tuberosities, and by cutting through the capsular ligament vertically, so as to follow it up to its attachment to the upper edge of the glenoid cavity, when it may be easily drawn aside with a blunt hook, until the operation has been completed—a proceeding difficult of accomplishment in old cases of disease or injury, and in them not necessary nor advisable.
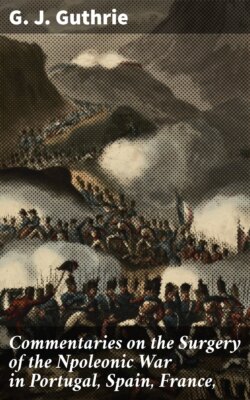
The accompanying sketch shows the head of the humerus of the right arm or side, with a ball lodged in it, a relic from Inkerman, sent to me as an especial mark of attention by one of the medical officers at Scutari, but without the name of the man, the regiment he belonged to, or the surgeon who performed the operation for its removal. The following account was wrapped round the bone. It commences a day or two after the operation was done at Scutari, and shows that the man died from an affection of the lungs, not uncommon, as was first shown during the late war, after operations following extensive suppurations:—
a. The head of the humerus sawn off below the tuberosities. b. The ball. c c. Fractures of the head of the bone.
“Pulse soft, 120. He passed a rather restless night, although he had another opiate at one A.M., and partially removed the dressings. In the morning he was better; he took some tea and a little wine with arrow-root, but was very much depressed in spirits. The wound looked well, there being less discharge, and of a more healthy character; no increased inflammation around the wound, but no tendency to union by the first intention on removal of the stitches. He was put upon farinaceous diet, with four ounces of wine and beef-tea. He continued to do well till the evening of the 16th, when he complained of tightness of the chest and slight cough. Harshness of respiratory murmur and increased vocal resonance, but no crepitation, could be detected on the right side on auscultation; he complained also of pain in the hypogastrium and slight diarrhœa. At bedtime he had a sedative antimonial draught, after which he rested well, but perspired profusely. On being particularly questioned, he admitted that he had had diarrhœa several times since landing at Varna, and had had bloody stools after the battle of Alma, for which, however, he had never been off duty; he had also frequently been troubled with cough, and two of his family, he understood, died of consumption. For two days he continued to improve in spirits, to take his food better, and the wound assumed a healthy granulating appearance, but a very small portion of the end of the humerus appeared white, as if going to necrose. On the evening of the 18th his breathing was more oppressed, and his countenance flushed and anxious. On examination of the chest, the lower two-thirds of the right lung were dull on percussion; bronchial breathing in the lower half, with crepitation above; in the left lung loud sub-crepitus; diarrhœa had also supervened during the day, but was checked for the time by an opiate enema. From this date his strength gradually sank; the diarrhœa returned again and again, in spite of repeated opiate enemata and small doses of Dover’s powder with hyd. c. cretâ. The surface of the wound assumed a less healthy appearance; the respiration became more labored, and he gradually sank till Saturday, November the 25th, when he died at half-past ten A.M.
“On examination of the head of the bone, after its removal, there was found an irregular, rugged cavity in the cancellated tissue, about an inch long, by half an inch broad, extending nearly transversely from the smaller to the greater tuberosity, and above the latter a musket-ball was found deeply imbedded, its external convex surface being on a level with the articular cartilage. From this several small fissures radiated over the globular head, and from each end of the cavity a much deeper one extended round the anatomical neck, separating the articular portion of the bone, in two-thirds of its circumference, from the shaft.
“At the post-mortem examination, the surface of the wound looked black and sloughy near the seat of injury, but more healthy in the direction of the incisions. A small portion of the end of the humerus was of a pearly white, in progress of necrosing; but around the shaft, immediately below this, and in the glenoid cavity, the process of repair had commenced. Both lungs were found engorged with frothy serum; the lower two-thirds of the right lung hepatized; traces of old tubercle in apices of both lungs, with miliary tubercle scattered throughout the whole substance of the left and upper part of the right. The whole tract of the colon, from the cæcum to the rectum, presented traces of ulceration, the ulcers being seldom larger than a split pea, with hardened, elevated edges; the bases in some instances were formed by the peritoneum only; generally they were scattered irregularly, but occasionally they were found in rows corresponding to the long diameter of the gut. In the rectum the ulceration was more extensive, in some parts the size of a farthing, the edges very irregular, and the direction more transverse.” These appearances precisely resemble those observed during the autopsy in cases of death from consumption, and are not therefore peculiar to the dysentery under which he had suffered.”
117. Professor B. Langenbeck, in order to save the deltoid muscle, proposed and practiced the operation in the following manner, during the Danish war in Sleswick-Holstein, with success in several instances: Begin the incision through the integuments and deltoid muscle immediately below the anterior border of the acromion, and continue it directly downward, over the minor tuberosity of the humerus, to the extent of four inches. Separate the parts, open the sheath of the long tendon of the biceps muscle, and draw out and hold it on one side with a blunt hook. Rotate the arm outward, (if it will rotate,) to facilitate the division of the tendon of the sub-scapularis; then rotate the arm inward, to aid in the division of the tendons of the supra-spinatus, infra-spinatus, and teres minor muscles, inserted into the great tuberosity. Complete the division of the capsular ligament, push the bone through from below, using the arm as a lever if you can, and saw it off. No arteries of consequence are wounded.
This operation would not be so easy of execution as is supposed, in cases in which the head and neck of the humerus are broken from the shaft; it would be very difficult of execution in old cases in which the soft parts are so hardened and impacted as to admit of little or no motion.
The extent to which the shaft of the humerus may be removed with the head cannot be distinctly defined. The greater the distance, the less will be the chance of the bone uniting to the glenoid cavity, in such a manner as to render it a useful limb, whether by the formation of a ginglymoid joint, or by anchylosis. In the present state of our knowledge the bone should not be sawn lower than the insertion of the deltoid muscle. If the arm were preserved by an operation below that part, it is probable that the bone, however supported, would not become attached to the glenoid cavity. It might however become useful, by some artificial help, as has occurred in cases of false joint in the middle arm, after ununited fractures.
118. Excision of the head of the humerus is not to be done in every instance of compound fracture of that bone, as the following cases will show:—
Lieutenant Madden, 52d Regiment, was wounded at the assault of Badajos in 1812, by a musket-ball, which fractured the head of the humerus, and lodged in it. The broken pieces were from time to time removed by incisions, together with the ball, and he ultimately preserved a very serviceable arm. He is now a very zealous member of the Church of England.
Robert Masters, 40th Regiment, was wounded at the battle of Toulouse, on the 12th of April, 1814, by a musket-ball in the right shoulder, which lodged in the head of the bone. Shown to me a few days afterward as a case for amputation at the shoulder-joint, I directed the excision of the head of the bone as soon as the parts became more quiescent. Under venesection, purgatives, leeches, the constant application of cold, and low diet, the high inflammatory symptoms which had supervened subsided, and, six weeks after the accident, the ball, and part of the head of the humerus, were removed, after an incision had been made through the external parts for the purpose. Three mouths after the receipt of the injury, the man was sent to England, with no other inconvenience than that resulting from the loss of motion in the shoulder, which was stiff. The use of the forearm was preserved, and a limited one of the upper arm, by moving the shoulder-bone on the trunk.
Private Oxley, 23d Regiment, was wounded at the battle of Toulouse, in April, 1814, by a musket-ball, which entered at the anterior edge of the deltoid muscle, passed across the head of the humerus, injuring it in its course, and went out near the posterior edge of the muscle, through which, at its middle part, the deficiency in the rotundity of the head of the humerus could be distinctly felt. Shown to me a few days afterward as a slight but peculiar wound, it was marked as a case for excision, if circumstances should render it necessary. No bad symptoms, however, supervened; the man only complained of the restraint put upon him, and the lowness of his diet. Some pieces of bone came away, or were removed, and in July he was sent to England, the wound being healed and free from pain; the shoulder stiff. The lower arm he used as before the accident.
General Lord Seaton suffered from a nearly similar wound, at the taking of Ciudad Rodrigo, and recovered with a good use of his arm.
These cases were fortunate in their results, but such do not always follow. Major C. was wounded in one of the battles in the Pyrenees, in 1813, by a musket-ball, which injured the head of the left humerus from side to side. Thirty years afterward the wounds still discharged, and gave him great uneasiness. A probe discovered much diseased bone. I advised the excision of the head of the bone, to which he would not assent. His courage had been broken by continued suffering.
Ensign Moore, of the Bengal army, was wounded at Sobraon, on the 10th February, 1846, by a musket-ball, which passed through the anterior and inner part of the deltoid muscle, one inch and a half below the inner part of the acromion process, struck and went through the head of the bone, which it splintered, and made its exit behind, in front of, but near the inferior angle of the scapula. He remained in camp three days, and was sent to hospital at Ferozapore, where he suffered much from inflammation, pain, etc., and after a month was sent to Subaltro in the Hills, where some pieces of bone came away, during which time he suffered severely, and was much weakened by it and the discharge. On the 20th October, 1846, he was removed to Bunda, in Bundeleund; here more bone came away, accompanied by much discharge. Thence he proceeded in April, 1847, to Juanpore, where he suffered three attacks of inflammation, two of them very severe; the constitutional disturbance was great. The posterior wound was reopened, and a large quantity of offensive matter discharged. On the 7th of August, 1847, the suppuration is stated to have been still great, and the strength very much reduced, on which account he was recommended to proceed to Europe. On the 9th June, 1848, the wounds were healed, the last piece of bone having come away about ten days before. The pieces of bone are from the head and from the part adjoining. The head of the bone is greatly diminished in size, so much so as to appear to have been almost entirely removed; the joint is stiff, if not anchylosed, the shoulder flat, the under use of the arm perfect, that of the upper part dependent on the motion of the shoulder-blade. The removal of the head of the bone, immediately after the receipt of the injury, would have been the best course to have pursued, for the arm when the cure took place was not in a better state than it would have been in if the operation had been performed at first, and the patient would have been spared two years of great suffering, not unattended with considerable danger.
M. Baudens, in a very able paper, an extract of which, made by himself, is published in the “Comptes Rendus” of the French Academy of Sciences, for February, 1855, on the Resection of the Head of the Humerus, seems to have overlooked, or not to have seen, the foregoing observations, as he assumes, as a consequence of his own observations on fourteen primary cases of which one only died, that the resection of the head of the humerus ought to be the rule in surgery when a ball has broken this part, and that amputation of the limb should be the exception—a point long since settled in my surgical works.
He considers that surgical writers in general have supposed that the bone remains suspended in the middle of the muscles, which does not accord with his practice, nor with the remarks made by me on this subject.
He recommends the following mode of operating: The arm being slightly turned outward and backward, the point of a small, straight amputating knife is to be entered on the outside of the coracoid process, immediately over the head of the humerus; lower the hand and carry the point of the knife in a straight line for ten or twelve centimeters downward, always applied to the bone, which serves as a guide.
If the incision thus made should not be large enough to expose the head of the humerus, a transverse subcutaneous one should be made through the muscular fibers toward the superior angle. If it be sufficiently large and open, this is not necessary. The long tendon of the biceps will be seen at the bottom of the incision, and is to be cut across.
Bring opposite the incision, by rotating the arm, first the great tuberosity, then the smaller one, in order to divide the four muscles attached to them. The division of these parts will largely open the joint, when the elbow being carried backward and upward, the head of the bone will protrude. Detach gently the periosteum, slip the chain saw behind and below the head of the bone, so as to leave the periosteum as much uninjured as possible, doing in fact a sub-periosteal extirpation.
Tie the vessels, cover the upper end of the humerus with the periosteum thus saved like a hood, and keep it in contact with the glenoid cavity.
He maintains that when a ball has broken the head of the humerus, if the removal of the head be not effected, one of three things follows: the operation is performed subsequently, or the patient dies of purulent deposits, or recovers with a stiff joint, accompanied by fistulous openings of a disagreeable nature.
He contends that a ginglymoid joint is always formed by his method, which enables the sufferer to make much greater use of it than if the operation were performed in any other way; but it will be very difficult of performance if the bone should be so much injured as to prevent the tuberosity following the motion to be given to the elbow, and is not therefore recommended.
119. If, from some complication of injury, the axillary or other artery should give way during the treatment, the extremity is not to be amputated. The artery is to be secured by one ligature applied above the opening in it and by another below it, the surgeon always bearing in mind the fact that the proper way to get at the axillary artery is by cutting across the fibers of the pectoral muscle, and not in their direction, and that it will be better to amputate the arm than to tie the subclavian artery above the clavicle.
120. Amputation of the arm by the common circular incision should only be practiced in the space between the lower edge of the insertion of the pectoralis major and the elbow-joint; and rarely in cases of injury from musket-balls. No common flesh-wound, made either by cannon or musket-shot, even including a division of the artery, absolutely demands this operation, the bone being uninjured. If, in addition to a destructive flesh-wound, the bone be broken, or if it be mashed with the muscles by an oblique stroke of a round shot, or the forearm be carried away or destroyed, it is admissible. It is to be done in the following manner: An assistant draws up the integuments with both hands; another does the same downward, if the parts admit of it; the forearm is to be moderately bent. The integuments are to be divided by a circular incision, and retracted. The muscles and vessels are then to be cut through by one sweep of the knife, if it can be done. The muscles adhering to the bone are next to be separated from it to the extent of two inches. The retractor is to be applied, and the periosteum divided by one circle of the knife around the bone, and in the circle thus cut the saw is to work until the bone is divided; attention being paid to the directions already given to saw in a perpendicular, not slanting direction. The artery or arteries are to be tied, the surface of the stump cleansed with warm and then with cold water, and dried. Leaden sutures are useful.
121. Mr. Luke performs the operation by two flaps on the same principle as in the thigh. There is a close resemblance in the manner of amputating the arm by the double-flap operation to that adopted for the amputation of the thigh. The first flap is made posteriorly to the bone, by transfixing the limb, for which purpose the knife is entered at the mid-point between the anterior and posterior surfaces, carried transversely across the limb, and made to cut toward the posterior surface, in an oblique direction, until all the soft structures are divided. It is necessary, in entering the knife, to bear in mind that the bone lies opposite to the mid-point, and that, in carrying the knife across the limb, it would strike against the surface of the bone, unless means were adopted for its prevention. This is easily done by grasping the structures which are to form the posterior flap between the fingers and thumb of the left hand, and by drawing them backward during the time the knife is entering at the mid-point and being carried across the limb. Having formed the posterior flap, the anterior one is formed as in amputation of the thigh, by cutting inward from the surface toward the bone with a sweep, which will make this flap equal in length to the posterior. The operation is completed by dividing the remaining soft parts by means of a cut carried circularly around the bone, and by sawing the bone in the line of division. The after-treatment is the same as in the thigh.
122. Excision of the elbow-joint.—An incised wound of moderate extent into the elbow-joint, cutting off with it a part of the condyle of the humerus, or the head of the radius, or a part of the ulna, demands the removal of the injured piece of bone only. The forearm should be bent, and the antiphlogistic treatment fully carried out. A ball fracturing the olecranon, or other portion of a single bone, although opening into the joint, does not immediately require any operation.
If a ball should lodge in the lower part of the humerus, or in either of its condyles, it should be removed as quickly as possible by the trephine, or other appropriate instrument.
When the articulating ends of the humerus, radius, and ulna are wholly or in part injured by a musket-ball, it was formerly the custom to amputate the arm in such instances of great mischief—an operation which should be superseded by that of excision of the joint, by which the forearm will be saved, and considerable use of it retained.
To perform this operation, a straight, strong-pointed knife is to be pushed into the joint behind, immediately above but close to the olecranon process, and exactly at its inner edge, to avoid the ulnar nerve, which lies between it and the inner condyle, to which it may be considered to be affixed. The incision thus begun is to be carried outwardly to the external part of the humerus, dividing the insertion of the triceps. At each end of this transverse cut an incision is to be made upward and downward for about two inches each way, the three resembling the letter H. The flaps thus made being turned up and down, the olecranon should be sawn across, together with the great sigmoid cavity and the coronoid process of the ulna, the insertion of the brachialis internus having been previously separated from the coronoid process. Before this is done, the ulnar nerve should be separated with its attachments from the inner condyle, and turned aside to avoid injury. The joint being now fully exposed, the head of the radius may be sawn off or cut through with the strong spring scissors if possible, above the tubercle into which the biceps tendon is inserted. The extremity of the humerus should next be pushed through the wound, and the broken end sawn off, a spatula or other thin solid substance being placed underneath it, to prevent the brachial artery or median nerve being injured. Any hemorrhage which there may be having ceased, the forearm is to be bent, the bones are to be placed in apposition, and the incisions approximated by sutures and sticking-plaster, duly supported by compress and bandage, so that union may take place if possible, particularly of the transverse wound first made. The arm should be supported by a sling, and dressed early, as the shot-hole or holes must remain open and discharging. Some motion of the new joint to be formed may be expected under gentle passive movements; but as a stiff joint cannot always be avoided, the arm should be kept bent.
123. Amputation of the elbow-joint has been recommended, but not frequently performed. It may be done in any way by which good covering can be obtained, and it has been supposed that the long stump thus made is more useful if the olecranon process be sawn across, and left with the triceps attached to it, than if it be removed. When the parts are sound, a flap may be made in front by introducing a straight, double-edged knife over the outer condyle, and carrying it across and through the soft parts over the opposite or inner condyle, when by cutting downward and outward a flap is to be formed of from three to four fingers’ breadth in length. A shorter flap is to be made behind, when both are to be raised, and the bleeding vessels previously secured, the external lateral ligament being divided. The radius is to be separated from the humerus, when the olecranon may be sawn across, or, if the arm be bent, separated from the humerus without difficulty. The flaps are to be brought together and retained in the usual manner.
124. Amputation of the forearm is seldom required after wounds from musket-balls. The bones can be readily got at, and large pieces removed with ease. The arteries can be cut down upon and secured without difficulty, except at the upper part, and even there with some little sacrifice of muscular parts, which are not to be spared. The fascia may be divided freely in every direction, and as mortification from defect of nourishment rarely takes place in the fingers, as it does in the toes, when the great arteries of the limb have been injured, every effort should be made to save a forearm, however badly it may at first appear to be injured.
The flap operation is to be preferred to the circular, particularly when done a little above the wrist; to which operation Baron Larrey and the surgeons of France particularly objected during the late war. Having done it most successfully since 1806, however, it is recommended as preferable to any other, even when the injury admits of its being done neat the carpus. When the nature of the injury does not admit of two equal flaps being formed, it must be done by two unequal ones, or even by one, it being important for the fixing of an artificial hand or other help to have a long stump.
The arm being placed and held firmly in the intermediate position between pronation and supination, with the thumb uppermost, so that the radius and ulna are in one line, a sharp-pointed straight knife is to be entered close to the inner edge of the radius, and brought out below at the inner edge of the ulna. It is then to be carried forward for half an inch, and made to cut its way out with a gentle inclination, so as to form a semicircular flap. Re-entered at the same point as before, a similar flap is to be made on the outside, the position of the bones being a little altered to admit of its easy execution. The two flaps are to be turned back; the tendon of the supinator radii longus, and all other tendinous, muscular, or interosseous fibers, not cut through, are then to be divided, and the linen retractor run between the bones, which are to be sawn across at the same time. All pressure being taken off, the tendons and the vessels, if long, are to be cut short, and the arteries to be tied, after which the flaps are to be brought together by sutures, and retained by sticking-plaster, compress, and bandage.
125. When the operation is to be performed above the middle of the arm, it may be done by the circular incision.
The arm being placed with the thumb uppermost, an assistant should retract the integuments as much as possible, while the operator makes a circular incision through them. They are then to be drawn up for nearly an inch. The muscles on the inside of the arm should be divided by one slanting cut to the bones; then those on the outside. The bones are to be cleared by cutting through any muscular fibers attached to them, when the interosseal ligament should be divided, and the linen retractor passed between the bones, which may be sawn through at the same time without difficulty. The stump is to be dressed in the usual manner. The operation may be done by cutting through the integuments and muscles at once in an oblique manner, until the flaps thus formed shall be sufficiently large to make a thick cushion over the ends of the bones.
126. Amputation at the wrist, or the joint of the radius and ulna with the first row of the bones of the carpus, has been recommended by some surgeons as preferable to amputation above the ends of the radius and ulna. The hand being placed midway between pronation and supination, the soft parts are to be divided by a circular incision beginning from half an inch to an inch below the ends of the radius and ulna. The integuments being turned up without the tendons, they are to be divided, and the joint is to be opened into before the spinous process of the radius; and, while the hand is pressed down, the knife should divide all the soft parts, and separate the carpus from the radius and ulna. The wound is to be closed by sutures in the usual manner. When a circular incision cannot be made, in consequence of the nature of the injury, and this operation is still preferred, a covering for the bones must be obtained wherever it can be procured, by one or more flaps.
127. In all injuries of the hand, the value of a thumb and a finger, or of two fingers, or even of one, should be borne in mind, and no part should be removed that can be saved, and appears likely to be of use. When cannon-shot, large splinters of shells, or grape-shot have struck the hand, amputation will often be necessary; but the foregoing precept should never be forgotten.
A musket-ball fairly passing through the hand generally fractures two metacarpal bones, although a small ball may pass between them without breaking either. The wounds should be enlarged, and the broken ends of the bone sawn off, or the splinters removed, and the points of bone smoothed off, the tendons to be carefully preserved, and vigorous antiphlogistic measures adopted. The tendency to tetanus or trismus will be best obviated by such measures, the incisions, when necessary, being made in the direction of the bones and tendons. Any hemorrhage which can ensue will be readily commanded by ligature, by torsion of the vessel, or by a small graduated compress and bandage, when those are inapplicable. Injuries by musket-balls to the metacarpal bones rarely take place without implicating one or more flexor or extensor tendons, and the consequence is that the fingers to which they belong are often bent inward toward the palm, constituting a defect less inconvenient, however, than if the finger remained straight and immovable.
128. When one or more fingers are destroyed, and the metacarpal bones injured, they are to be sawn or cut off, but not removed at the carpus, although an opening into the joint of the carpus will generally do well, if skin can be saved to cover it. In all cases of amputation of one or more fingers, the metacarpal bones, if injured, should be left as long as possible, and particularly that of the index finger, when the thumb remains. In all cases it is better, if possible, to leave the heads of the metacarpal bones in their places, rather than open into the joint of the carpus, if it can be avoided. If the articulating heads must come out, a strong, thin scalpel is to be pushed in between the bones, the ligaments cut through above, below, and at the sides, and care should be taken, in removing one or two of these bones, not to dislocate the others, and the joint should be covered by a flap or flaps made for the purpose, the sides of the remaining fingers being covered in a similar manner. This succeeds admirably, when the two outer bones and fingers only are taken away.
129. The phalanges of the fingers may be removed by making a flap from the upper or under part, or from both, or from the sides. The square flap from the upper part of the finger is preferable, when the joint with the metacarpal bone is to be operated upon, the commencing points of the flap being united by a transverse incision on the under part of the joint. It should be recollected, that in all these excisions the larger end of bone belongs to that which is not removed, as may be shown by bending the finger; and that the ligamentous attachment between the metacarpal bones, connecting a middle one to its fellows on each side, should be cut through, when the joint will be easily dislocated. Attention should be paid to the division of the lateral ligaments, in the removal of any of the bones of the fingers.
Professor B. Langenbeck has operated in some instances, and he says successfully, without the loss of the finger, by sawing off, in his first case, the articulating ends of the first phalanx and of the metacarpal bone of the forefinger, in consequence of an injury from a rotating piece of machinery; in another, the ends of the first and second phalanges of the middle finger after a severe laceration; and in a third case, by sawing off the end of the second phalanx, and removing the whole of the bone of the third of the forefinger from the soft parts, leaving the nail; the man recovering with a shortened but useful finger. In all these cases the flexor and extensor tendons were from the first uninjured.
M. Langenbeck has also removed the metacarpal bone of the thumb in the following manner: “An incision is to be made along the whole length of the bone toward the palmar aspect, thus avoiding the tendons. Then free both articulating extremities, separate the soft parts from the body of the bone, which is to be drawn outward by a strong pair of forceps, with two bent points or teeth at each extremity. To prevent the shortening or drawing inward of the thumb, it is to be kept straight and duly extended by a splint and other apparatus.” He recommends, with Flourens, the preservation of as much as possible of the periosteum, and uses for its detachment a small curved knife with a square end. Separating the periosteum from the bone is more easily directed than done. Professor Quekett, at my request, made some trials on the humerus to ascertain the point, and found that the periosteum could not be separated from the cartilaginous covering of the head of the bone, in the manner proposed, although it could be done by scraping half an inch below the insertion of the capsular ligament, and a sufficient portion saved to cover the sawn end of the bone, in the manner recommended by M. Baudens.