Читать книгу Physiologically Based Pharmacokinetic (PBPK) Modeling and Simulations - Sheila Annie Peters - Страница 52
2.3 FACTORS AFFECTING DDI
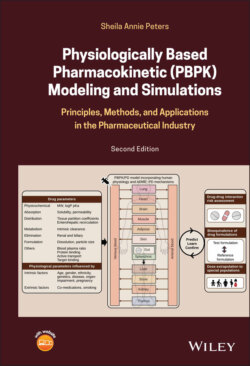
ОглавлениеThe extent of DDI will depend on the characteristics of the perpetrator and victim drugs involved in the interaction. Perpetrator and victim properties impacting drug interaction risk are summarized in Figure 2.2. For an inhibitor, the greater the unbound inhibitor concentration relative to its potency, the greater is the extent of inhibition. Inhibitor concentrations at any point of time will depend on the dose administered and the organ where the affected enzyme or transporter is located. For a victim of inhibition, the greater its dependence on the inhibited route for its elimination, the greater is the potential for an altered pharmacokinetics of the drug. If more than 70% of a drug is eliminated using the inhibited pathway, the risk for interaction is high (Dunne et al., 2011). Thus, it is important to balance the clearance of a victim drug between hepatic, renal, and biliary routes during the design stage, in order to minimize risk from drug–drug interactions. For a high clearance victim drug that is orally administered, the magnitude of interaction is likely to be high due to first‐pass, making it more sensitive to DDI compared with a low clearance drug. Victim drugs associated with a narrow therapeutic window and high variability are more sensitive to DDI.
Figure 2.2. Perpetrator and victim properties impacting drug interaction risk.
Induction and/or inhibition of drug transporters of the small intestine, liver, and kidney are major determinants of drug–drug interactions. Transporter‐mediated drug–drug interactions in these three organs can considerably influence the pharmacokinetics and clinical effects of drugs. Transporters of interest are those controlling intestinal efflux, hepatic efflux, blood–brain barrier (P‐gp and BCRP), hepatic uptake (OATP1B1 and OATP1B3) and renal tubular uptake/bidirectional transport (OAT1, OAT3, OCT2), and efflux (MATE1 and MATE2/K). Renal DDIs are rare and associated with significantly lower AUC ratios compared with hepatic DDIs. Victims of renal DDIs are generally compounds whose eliminations are largely dependent on the renal route. Examples include metformin, a substrate of OCT2 and MATEs, and the endogenous compound creatinine, a substrate of OAT2, OCT2, and MATEs, the secretion of both of which are reduced by cimetidine, known to inhibit OCT2 and MATEs. Cimetidine also reduces the renal clearance of bisoprolol, nicotine, and procainamide (Ayrton and Morgan, 2001; Shitara et al., 2009; Shitara et al., 2009; Kirch et al., 1987; Somogyi et al., 1987; Bendayan et al., 1990; Ayrton and Morgan, 2001; Shitara et al., 2009; Ivanyuk et al., 2017). Uptake transporters act in concert with efflux transporters to eliminate toxins (e.g., OCT2 and MATE1, MATE2‐K). Therefore, for secreted drugs that are reliant on transporters for overcoming the membrane barrier, the inhibition of efflux transporters could result in an accumulation of drugs in the cytoplasm of proximal tubular cells, leading to toxic effects in the kidney (nephrotoxicity). Perpetrators of renal DDIs are usually acids or bases with high therapeutic doses and inhibit the renal uptake transporters OATs 1 and 3 or OCT2. Probenecid inhibits the renal OATs and causes drug–drug interactions when coadministered with hydrophilic acids that are predominantly cleared by the kidney, such as penicillin, famotidine, and chlorothiazide (Inotsume et al., 1990; Ayrton and Morgan, 2001; Ho and Kim, 2005; Shitara et al., 2009). Decreases in renal function with age and disease will impact the extent of drug interaction.
Complex drug–drug interactions (DDIs) with potential involvement of multiple elimination pathways and interaction mechanisms is challenging. When a transporter and an enzyme are involved in DDI, then the net effect depends on whether the inhibitor or the substrate of the enzyme is dependent on the transporter for access to the enzyme. Understanding the mechanisms underlying complex DDIs are challenged by the lack of specific probe substrates for transporters (Jones et al., 2020). Rifampicin through its activation of the nuclear receptor, PXR, induces CYP3A4. Additionally, it also inhibits OATP1B1 uptake transporter. Thus, a single dose of rifampicin caused an 8‐fold increase in the in the exposure of atorvastatin (Lau et al., 2007) However, multiple doses of rifampicin caused a decrease in the exposure of atorvastatin, due to induction (Backman et al., 2005). When multiple inhibitors inhibit multiple enzymes, the overall effect is additive, but if they inhibit the same enzyme, then the net effect defaults to the most potent inhibitor.