Читать книгу Recent Advances in Dialysis Therapy in Japan - Группа авторов - Страница 25
На сайте Литреса книга снята с продажи.
HD Cycle and Onset of SCD
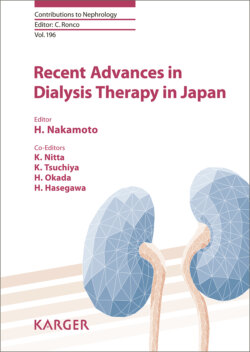
ОглавлениеPropensity of the time of onset of SCD in the HD cycle provides a hint as to the risk factors and triggers for SCD. Several studies [20–22] have already demonstrated a strong association between a long interdialysis interval and cardiac mortality and hospitalization in HD patients in the routine clinical setting. These findings demonstrated that SCD is more likely to occur on Monday for HD patients receiving treatment on a Monday, Wednesday, and Friday cycle, and on Tuesday for those with a Tuesday, Thursday, and Saturday cycle. However, which timing, pre- or post-HD after a long interval, carries a greater likelihood of SCD is not clear, though the study by Bleyer et al. [23] may provide the answer. They examined the risk of sudden death for each 12-h interval from the start of HD. As shown in Figure 1, the highest risk was seen within 12 h before HD after a long interval, and then the second highest risk was found in the 12 h during and after each HD treatment. Surprisingly, a not so high risk for sudden death was observed in the 12 h before HD after a short interval. These findings suggest that the pre-HD period after a long interval and every post-HD period are high-risk zones for SCD. It is noteworthy that post-HD occurs three times more often than pre-HD after a long interval.
Fig. 1. The ratio of observed to expected death proportions for each 12-h time interval of the weekly HD cycle. The highest ratio (about 3) is found in the 60–72 h from the beginning of HD. The second highest ratio (about 1.7) is observed in the 12 h beginning with dialysis treatment, which includes the time during and following hemodialysis. From Bleyer et al. [23].
Is the type of fatal arrhythmia responsible for SCD difference between pre- and post-HD? Although there is no good answer to this question, the differences in the characteristics of SCA have been investigated in HD patients [24]. Studies have compared the characteristics of SCA between two patient groups, those with and without VF. SCA from VF was more often seen in the post-HD period, while SCA from non-VF, which may be bradyarrhythmia, was more often seen in the pre-HD period. This may imply that the cause of SCA in HD patients is bradyarrhythmia due to hyperkalemia in the pre-HD period after a long interval and fatal ventricular arrhythmia due to a long QT interval in the post-HD period. Because some recent evidence suggests that shifts of electrolytes, such as potassium and calcium, during HD cause a rapid prolongation of the QT interval after HD, this may lead to the onset of ventricular arrhythmia and SCD. This may be one of the major potential causes of SCD during and after HD.