Читать книгу Recent Advances in Dialysis Therapy in Japan - Группа авторов - Страница 26
На сайте Литреса книга снята с продажи.
Long QT Interval due to Dialysis Solution
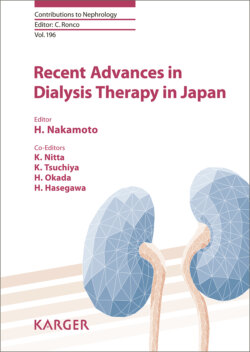
ОглавлениеA prolonged QT interval on ECG is a well-known risk factor for fatal ventricular arrhythmias such as Torsades de Pointes and, consequently, the onset of SCD [25]. It has been recently reported that there is a high prevalence of HD patients with corrected QT (QTc) prolongation [26]. Niemeijer et al. [27] demonstrated that about 65% of Chinese HD patients had a prolonged QTc, defined as greater than 440 ms for males and greater than 460 ms for females, on pre-HD electrocardiograms. It is well established that QTc prolongation can be caused by the presence of cardiac diseases, such as coronary heart disease and heart failure, and it is usually caused by certain drugs. On the other hand, several studies have shed light on the importance of electrolyte levels, especially calcium and potassium levels, and their shifts for the development of QT prolongation and SCD in HD patients. It has been reported that QTc is affected by the differences in calcium and potassium concentrations in dialysis fluid. QTc in the post-HD period was longer with the combination of low calcium (2.5 mEq/L) and low potassium (2.0 mEq/L) in dialysis fluid than with the combination of high calcium (3.5 mEq/L) and high potassium (3.0 mEq/L) [28]. A significant linear negative correlation was observed between the delta change of calcium and the delta change of QTc during HD (Fig. 2). This correlation was stronger than the correlation of potassium change with QTc change. This suggests that calcium shifts during HD have a greater impact than potassium shifts on the development of QTc prolongation in HD patients. It should be noted that QTc was longer 4 h after HD even though calcium levels increased from pre- to post-HD. These findings suggest that, rather than an absolute calcium decrement during HD, a calcium gradient may have a greater impact on QTc prolongation. It has been reported that dialysate calcium concentration <2.5 mEq/L was associated with a two-times increased risk of SCD [29]. A lower dialysate calcium concentration may increase the gradient of the ionized calcium level, which may induce QTc prolongation, consequently increasing the risk for fatal ventricular arrhythmia. Actually, in the same study, a higher calcium gradient, which was defined as the difference between the pre-HD corrected total serum calcium level and the dialysate calcium level, was associated with a higher risk of SCD in HD patients [29]. Finally, it is also important to remember that the bicarbonate concentration in dialysate can affect QTc prolongation. Di Iorio et al. [30] demonstrated that changes in QTc were correlated with the bicarbonate concentration, and the combination of low calcium (2.5 mEq/L), low potassium (2.0 mEq/L), and high bicarbonate (34 mEq/L) dialysate was independently associated with prolongations in the QTc interval at the end of HD. The changes in QTc were constantly longer with dialysate containing high bicarbonate, whatever the concentrations of calcium and potassium. It is well known that there is an inverse association between pH and ionized calcium [31]. The effects of high bicarbonate dialysate on ionized calcium may be more intense when the dialysate calcium concentration is lower [30].
Fig. 2. Scatter plots of potassium, calcium, and QTc changes calculated by end-dialysis values minus predialysis values. The hourly changes in the QTc interval during the HD sessions are inversely correlated with the changes in plasma and ionized calcium concentrations. The correlation between changes in the plasma potassium concentration and changes in the QT interval is weaker than that of the plasma and ionized calcium concentration. From Genovesi et al. [28].